Acanthosis nigricans
|
Introduction |
|
Acanthosis nigricans (AN) is characterized by dark, coarse
and thickened skin with a velvety texture, being symmetrically distributed on
the neck, the axillae, antecubital and popliteal fossae, and groin folds,
histopathologically characterized by papillomatosis and hyperkeratosis of the
skin.
Two main forms exist: benign and malignant
forms.In the benign form of acanthosis nigricans, the factor is probably
insulin or insulin like growth factor (IGF). Other proposed mediators include
other tyrosine kinase receptors (epidermal growth factor receptor [EGFR] or
fibroblast growth factor receptor [FGFR]).
At high concentrations, insulin may exert potent
proliferative effects via high-affinity binding to IGF-1 receptors. In addition,
free IGF-1 levels may be elevated in obese patients with hyperinsulinemia.
In malignant acanthosis nigricans, the
stimulating factor is hypothesized to be a substance secreted by the tumor.
Transforming growth factor (TGF)–alpha is structurally similar to epidermal
growth factor and is a likely candidate. Reports of urine and serum TGF-alpha
levels normalizing after surgical tumor removal exist, with subsequent
regression of skin lesions.
Epidemiology
AN can occur at any age. The benign form is most common in
adults but also common in obese children. The malignant form, which is rare,
usually arises in older age groups >40 years.
Predisposing
factors
AN is associated with a number of benign and
malignant conditions with a common pathway of keratinocyte and fibroblast
proliferation by circulating factors. Perspiration or frictions are mechanical
contributing factors, as suggested by the predilection of acanthosis nigricans
for body folds.
Clinical features
Acanthosis nigricans is
characterized by dark, coarse, thickened skin with a velvety texture. The
earliest change is grey-brown/black pigmentation that is palpably thickened and
covered by small papillomatous elevations, giving it a velvety texture. As
thickening increases, skin lines are further accentuated and the surface
becomes mammilated and rugose, with the development of larger warty
excrescences. Acrochordons (skin
tags) are often found in and around the affected areas. AN is usually asymptomatic, but occasionally, it can be pruritic. The
lesions are symmetrically distributed on the back and sides of neck, axillae,
groin, and antecubital and popliteal areas. Neck is the most common
site affected (99%) in children when compared with axillae (73%). Face,
extensor surface of elbows and knees, dorsa of joints of hands, umbilicus,
external genitalia, inner aspects of thighs and anus are also
involved. With extensive involvement, lesions can be found over the
areolae, and eye, including papillomatous lesions on the eyelids and
conjunctiva. Involvement of mucous membranes is
uncommon, but oral mucous membrane may show delicate velvety
furrows. Generalized involvement can be a rare manifestation of
certain types of AN, being common in adults with underlying malignancy. When on
the face, it should be considered in the differential diagnosis of facial
hyperpigmentation. On the face, AN presents as poorly demarcated hyperpigmentation
with a predilection for the malar region inferior to the zygoma and the
nasolabial folds, and has even been described on the supraalar creases.
Recognizing this entity is becoming steadily more important as the rates of
obesity and non-insulin-dependent diabetes increases. Tripe palms presents as
rugose hyperkeratosis and prominent dermatoglyphics of palms, likened to bovine
gut lining. It is paraneoplastic in occurrence associated with malignancy in
90%, gastric cancer being the most frequent.
Clinical variants
Nine types of
acanthosis nigricans have been described.
Obesity-associated
acanthosis nigricans
Obesity-associated acanthosis nigricans,
once labeled pseudo–acanthosis nigricans, is the most common type of acanthosis
nigricans. Lesions may appear at any age but are more common in adulthood. More than half the adults who weigh >200% of their
ideal body weight have AN. The dermatosis is weight dependent, and
lesions may completely regress with weight reduction. Insulin resistance is
often present in these patients.
Syndromic acanthosis nigricans
Syndromic acanthosis nigricans is
the name given to acanthosis nigricans that is associated with a syndrome. The
type A syndrome and type B syndrome are special examples.
The type A syndrome also is termed
the hyperandrogenemia, insulin
resistance, and acanthosis nigricans syndrome (HAIR-AN syndrome). This
syndrome is often familial, affecting primarily young women. It is associated
with polycystic ovaries or signs of virilization (eg, hirsutism, clitoral
hypertrophy). High plasma testosterone levels are common.
Type B insulin resistance syndrome
is characterized by the association of AN with diabetes and hyperandrogenism,
or with an autoimmune disease (including systemic lupus erythematosus, systemic
sclerosis, Hashimoto thyroiditis and Sjögren syndrome). Circulating antibodies
to the insulin receptor may be present.
Acral acanthosis nigricans
Acral acanthosis nigricans occurs in
patients who are in otherwise good health and in dark-skinned individuals and
manifests as velvety thickening and hyperpigmentation of the skin on the dorsa
of the hands and feet, especially the knuckles.
Unilateral acanthosis nigricans
(Nevoid acanthosis nigricans)
It is a rare form of AN, inherited as an autosomal dominant
trait. Clinically, it appears as a
unilateral pigmented plaque, along a line of Blaschko, and resembles an
epidermal naevus and may become evident during
infancy, childhood, or adulthood. Unilateral nevoid AN is not related to
endocrinopathy.
Familial acanthosis nigricans
It is a rare autosomal dominant genodermatosis
beginning during early childhood. The condition often progresses until puberty
after which it stabilizes or regresses.
Generalized acanthosis
nigricans
Generalized acanthosis nigricans is
very rare, and seen only in children without underlying systemic disease or malignancy. There
is generalized hyperpigmenation and velvety thickening of the skin.
Drug-induced
acanthosis nigricans
This may appear as an
adverse effect of several medications that promote hyperinsulinemia, including pituitary
extract, systemic corticosteroids, testosterone and exogenous estrogens,
including oral contraceptives. Nicotinic acid is most widely recognized
association. The lesions of acanthosis nigricans may
regress following discontinuation of the offending medication. Erickson et al. first
described AN as a rare local cutaneous side-effect of insulin injection
likely due to activation of IGF receptors. Prescription of the correct insulin and use of proper
technique will prevent AN development.
Malignant acanthosis nigricans
Malignant acanthosis nigricans,
which is associated with internal malignancy, is the most worrisome of the
variants of acanthosis nigricans because the underlying neoplasm is often an
aggressive cancer.
Acanthosis nigricans has been
reported with many kinds of cancer, but, by far, the most common underlying
malignancy is a gastric adenocarcinoma.
In 25-50% of cases of malignant
acanthosis nigricans, the oral cavity is involved. The tongue and the lips are
most commonly affected, with elongation of the filiform papillae on the dorsal
and lateral surfaces of the tongue and multiple papillary lesions appearing on
the commissures of the lips.
Tripe palms may show altered
dermatoglyphics due to alteration of epidermal rete ridges
Malignant acanthosis nigricans is
clinically indistinguishable from the benign forms.
Papillomatous
lesions on the eyelids and conjunctiva may occur. Leukonychia and nail
hyperkeratosis has been reported. In one-third of cases skin changes occur
before signs of cancer, in another one-third AN and neoplasm arise
simultaneously and in remaining one third, skin findings manifest after
diagnosis of cancer. Warning signs that call for evaluation for
malignancy in AN patients include age >40 years, not having any previous
endocrine disorder or any genetically determined disease, unintentional weight
loss, rapid onset of extensive AN, higher rate of pruritus, atypical sites, tripe palms, florid
cutaneous papillomatosis, in which there is a rapid
development of numerous warty papules on the trunk and the extremities that are
clinically indistinguishable from viral warts
and sign of Leser-Trélat.
Regression of acanthosis nigricans
has been seen with treatment of the underlying malignancy, and reappearance may
suggest recurrence or metastasis of the primary tumor.
Malignant acanthosis nigricans might be explained by elevated
levels of transforming growth factor (TGF-α), exerting effects on epidermal
tissue through epidermal growth factor (EGF) receptor. TGF-α produced by cancer
cells is structurally similar to EGF-α, interacts with the same receptor on the
cell surface, probably binding with it in different sites. The receptor for EGF
is found on actively proliferating cells of the basal layer where it is
involved in growth and differentiation of normal keratinocytes. When these
growth factors are produced by the primary tumor and circulate in large
quantities, they may cause epidermal cell proliferation, leading to AN.
Mixed-type acanthosis nigricans
Mixed-type acanthosis nigricans
refers to those situations in which a patient with one of the above types of
acanthosis nigricans develops new lesions of a different etiology. An example
of this would be an overweight patient with obesity-associated acanthosis nigricans
who subsequently develops malignant acanthosis nigricans.
|
Pathogenesis |
|
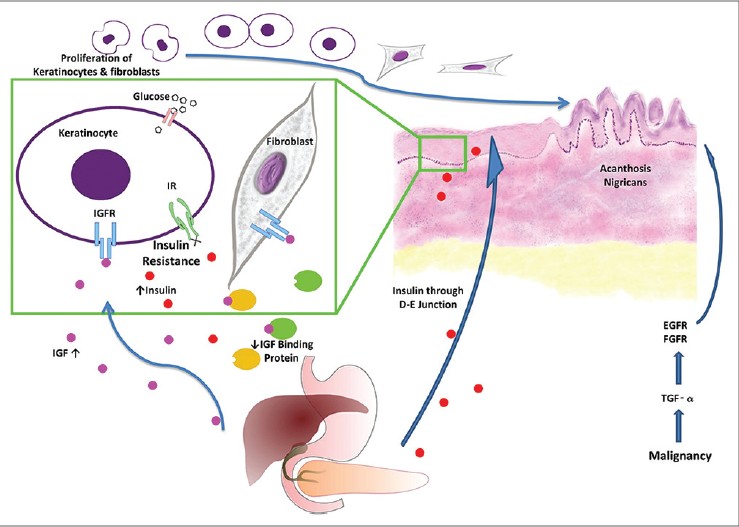
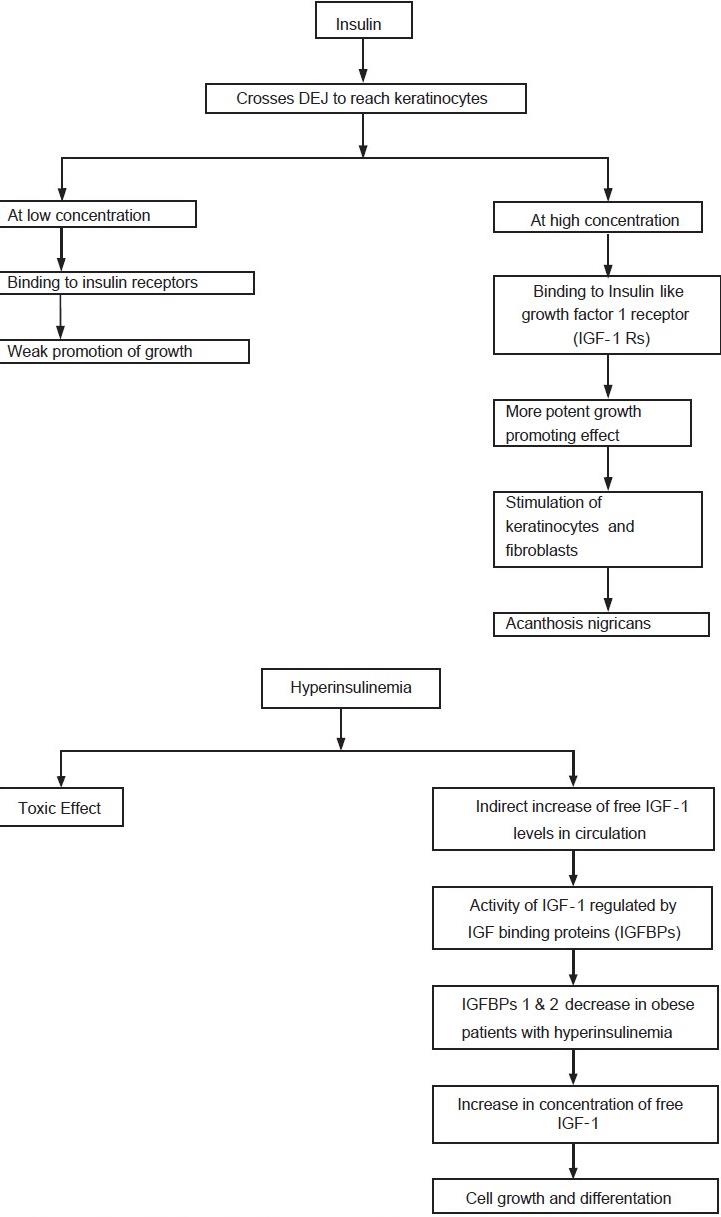
Insulin has been demonstrated to cross dermoepidermal junction (DEJ) to reach keratinocytes. At low concentrations, insulin regulates carbohydrate, lipid and protein metabolism and can weakly promote growth by binding to "classic" insulin receptors. At higher concentrations, however, insulin can exert more potent growth-promoting effects through binding to insulin-like growth factor 1 receptors (IGF-1Rs) that are similar in size and subunit structure to insulin receptors, but bind IGF-1 with 100- to 1000-fold greater affinity than insulin. The binding stimulates proliferation of keratinocytes and fibroblasts, leading to AN.
Hyperinsulinemia not only causes AN by exerting
a direct toxic effect, but indirectly by increasing free IGF-1 levels in
circulation. The activity of IGF-1 is regulated by insulin-like growth binding
proteins (IGFBPs), which increase IGF-1 half life, deliver IGFs to target
tissues and regulate levels of metabolically active "free" IGF-1.
IGFBP-1 and IGFBP-2 are both decreased in obese subjects with hyperinsulinemia,
increasing plasma concentrations of free IGF-1, which promotes cell growth and
differentiation [Flow Chart].
Insulin and IGF-1
levels are both may be implicated in etiogenesis of acrochordons and AN through
their proliferative and differentiating properties.
Insulin
resistance and AN

Insulin resistance is a metabolic disorder
in which target cells fail to respond to normal levels of circulating insulin,
resulting in compensatory hyperinsulinemia. IR has been associated with AN and acrochordons
which may represent an easily identifiable sign of IR and noninsulin-dependent
diabetes. AN is so closely associated with IR that it has been called a
clinical surrogate for laboratory determined hyperinsulinemia. Katie S in their
study observed that posterolateral neck texture had the highest sensitivity
(96%) for IR compared with neck/axillary texture and pigment and proposed the
term insulin neck (visibly increased texture on posterolateral neck appearing
as visible lines and/or furrows and ridges) for this finding. They suggested
that all patients with elevated BMI should be examined for insulin neck and if
neck texture is normal, IR is less likely to be present. IR occurs
in 20-25% of the individuals. Obese patients and patients with polycystic ovary
syndrome have Type A IR.
Acanthosis nigricans
and cardiovascular disease
Insulin resistance
is thought to be a primary etiological factor in the development of cardiac
dysfunction, higher prevalence being reported in non ischemic heart failure
population. It predates the development of cardiovascular disease and
independently defines a worse prognosis. Reduction in endothelial function may
be a link between IR and decline in cardiovascular performance.
Acanthosis nigricans and adipokines
Acanthosis nigricans patients have hyperinsulinemia
and may be at greater risk of atherosclerotic cardiovascular
disease. The commonest underlying cause of IR is excess abdominal
adipose tissue which releases increased amounts of free fatty acids which
directly affect insulin signaling, diminish glucose uptake in muscle, drive
exaggerated triglyceride synthesis and induce gluconeogenesis in liver. Other
factors presumed to play a role in IR are tumor necrosis factor α, adiponectin,
leptin, interlukin-6 and other adipokines. When β-cells fail to secrete excess
insulin needed, diabetes mellitus Type 2 and coronary heart disease occur as a
complication of IR.
Metabolic syndrome, insulin resistance and adipokines
Obesity is
commonly associated with type 2 diabetes, coronary artery disease, and
hypertension, coexistence of which is termed the metabolic syndrome. IR lies at
the heart of the metabolic syndrome. Elevated serum triglycerides commonly
associated with IR represent a valuable clinical marker of metabolic syndrome.
White adipose tissue is a major site of energy
storage and it has been increasingly recognized as an important endocrine organ
that secretes a number of biologically active "adipokines" (leptin,
adiponectin, resistin), some of which (especially resistin and adiponectin) have
been shown to directly or indirectly affect insulin sensitivity through
modulation of insulin signaling and the molecules involved in glucose and lipid
metabolism.
Chronic state of
IR is associated with secondary changes in levels of "adipokines"
(decreased serum adiponectin, increased serum resistin and decreased
adiponectin gene expression). Decrease in adiponectin levels by genetic and
environmental factors contributes to the development of the metabolic syndrome.
Adiponectin is important because of its antidiabetic and antiatherogenic
effects; hence it is expected to be a novel therapeutic tool for the metabolic
syndrome. The thiazolidinedione (TZD) class of antidiabetic drugs, having
pleiotropic effects on cardiovascular diseases and lipid metabolism exert their
effects partly through increasing levels of adiponectin. Adiponectin expression
and levels in circulation are upregulated by rosiglitazone.
Laboratory Studies
In
middle-aged and older patients with extensive skin or severe skin and mucosal
findings, a workup for internal malignancy is indicated.
The
vast majority of cases are due to obesity and/or insulin resistance. Screen for
diabetes with a glycosylated hemoglobin level or glucose tolerance test.
Screen for insulin resistance
A
good screening test for insulin resistance is a plasma insulin level, which
will be high in those with insulin resistance. This is the most sensitive test
to detect a metabolic abnormality of this kind because many younger patients do
not yet have overt diabetes mellitus and an abnormal glycosylated hemoglobin
level, but they do have a high plasma insulin level.
Glucose/insulin
ratio has been used in studies as an index of IR. It is a highly sensitive and
specific measurement of insulin sensitivity. In adults, a ratio of <4.5 is
abnormal, whereas in prepubertal children <7 is abnormal.
Histologic Findings
Histologic
examination reveals hyperkeratosis, papillomatosis, with minimal or no acanthosis.
The dermal papillae project upward as fingerlike projections. Clinical
hyperpigmentation is secondary to the hyperkeratosis and not to increased
melanocytes or increased melanin deposition. Dermal inflammatory infiltrate is
minimal or nonexistent. Mucosal acanthosis nigricans reveals epithelial
hyperkeratosis and papillomatosis along with parakeratosis.
Prognosis
The
prognosis for patients with malignant acanthosis nigricans is often poor. The
associated malignancy frequently is advanced, and the average survival of these
patients is approximately 2 years.
Patients
with the benign form of acanthosis nigricans experience very few, if any,
complications of their skin lesions. However, many of these patients have an
underlying insulin-resistant state that is the cause of their acanthosis nigricans.
The severity of skin findings may parallel the degree of insulin resistance,
and a partial resolution may occur with treatment of the insulin-resistant
state.
Treatment of AN
Management of AN is the management
of the underlying condition. In familial AN or AN not associated with an
underlying condition, treatment is aimed at improving the cosmetic appearance
of the condition.
Weight loss and
exercise have shown to increase insulin sensitivity and reduce insulin levels
causing improvement in obesity associated AN. Correction
of hyperinsulinemia reduces hyperkeratotic lesions.
Cessation
of the inciting agent in drug-induced acanthosis nigricans often results in
resolution. Dietary fish oil reportedly is beneficial in patients with
lipodystrophic diabetes and generalized acanthosis nigricans.
Topical treatment
Retinoids
Topical retinoid is considered first-line treatment, especially for unilateral
nevoid AN. It corrects hyperkeratosis and causes near
complete reversion to normal state. Intermittent tretinoin application is
needed to maintain improved status.
Combination of ammonium lactate and tretinoin
Retinoids affect cell growth, differentiation, and morphogenesis and alter cell
cohesiveness. Lactic acid is an alpha-hydroxy acid that works as a peeling
agent and also via release of desmogleins, indicating disintegration of
desmosomes. Though the exact mechanism of action of the two agents is unknown,
synergistic interaction is thought to play a role.
Peels
Trichloroacetic acid (TCA) is a superficial
chemical exfoliating agent causing destruction of the epidermis with subsequent
repair and rejuvenation. TCA (15%) is caustic and causes coagulation of skin
proteins leading to frosting. Precipitation of proteins leads to necrosis and
destruction of epidermis, followed by inflammation and activation of wound
repair mechanisms. This leads to re-epithelialization with replacement of
smoother skin. The advantages of TCA are that it is a stable product, hence
systemic absorption and peel depth correlate with the intensity of frost and
endpoint is easy to judge. TCA is safe, easily available, cheap, and easy to
prepare. TCA 15% is a safe and effective therapeutic modality for AN in
comparison to other topical treatments.
Calcipotriol
Calcipotriol is another beneficial
treatment in AN. It inhibits keratinocyte proliferation
and promotes differentiation by increasing intracellular calcium levels and
cyclic GMP levels in keratinocytes. Gregoriou et al.
concluded that it is safe, well-tolerated, alternative treatment for AN when an
etiological treatment is not possible or necessary. Bohm et al.
reported a case of mixed-type AN responding favorably to calcipotriol.
Oral treatment
Oral retinoids
Oral retinoids (isotretinoin, acitretin) can be effective; improvement
requires large doses and extended courses, and relapses are described. The
mechanism of action is probably normalization of epithelial growth and differentiation. Acitretin
has been rarely reported for AN treatment and has showed good success in cases
with syndromic and benign AN. Oral isotretinoin has been used successfully
treat to extensive AN.
Metformin and rosiglitazone
Metformin and rosiglitazone are useful in AN
characterized by IR. Paula et al. observed reduction in
fasting insulin levels with rosiglitazone when compared to metformin and modest
improvement of skin texture with both. Duration of treatment may be related to
improvement as metformin improves AN and IR if given for 6 months or more. Metformin
reduces glucose production by increasing peripheral insulin responsiveness,
reduces hyperinsulinemia, body weight and fat mass and improves insulin
sensitivity. The combined use of metformin and TZDs
which increase sensitivity to insulin in peripheral muscles, also give good
results.

Cosmetic treatment
Because
darkening of affected areas is common in AN, Alan Rosenbach considered the
possibility that long-pulsed alexandrite laser, which was designed to target
melanin in hair could improve this condition. They hypothesized that thermal
heating of epidermis and dermis results in tissue remodeling and pigment
reduction. They reported 95% clearance of AN of axillae after seven sessions
and concluded that long-pulsed alexandrite laser can effectively and safely
treat acanthosis nigricans of the axillae.
Treatment of malignant AN
Surgical removal of
tumors is the mainstay of treatment for malignant acanthosis nigricans, if
possible, because clearance following primary malignancy excision has been
described.
Conclusion
Though mainly a disease of cosmetic concern, AN can be
pointer to underlying metabolic syndrome or malignancy. A thorough
investigation and treatment is therefore mandatory to prevent long term
consequences.
Therapeutic ladder
First line
·
Topical retinoids – may reduce the
hyperkeratosis
Second line
·
Topical α‐hydroxyacids and keratolytics such
as salicylic acid may improve appearance by reducing hyperkeratosis
Third line
·
In extensive cases oral isotretinoin
has been used with some success

