Dermatitis
herpetiformis
Salient
features
· DH is a cutaneous
manifestation of celiac disease (CD) and is associated with gluten sensitivity
in virtually all cases
· DH and CD are genetic
disorders strongly associated with the HLA-DQ2 genotype, in which IgA
anti-endomysial antibodies are directed against tissue transglutaminase;
the presumed auto antigen within the skin is epidermal transglutaminase
· Both the intestinal
and cutaneous disease in DH can be controlled by gluten restriction; while only
cutaneous rash respond to sulfone therapy
Introduction
Dermatitis
herpetiformis is an inflammatory cutaneous disease with a chronic-relapsing
course, pruritic polymorphic lesions and typical histopathological and
immunopathological findings. There is growing evidence that dermatitis
herpetiformis should be considered the specific phenotypic cutaneous expression
of a gluten-sensitive enteropathy indistinguishable from celiac disease. Although over 90% of DH patients have evidence of a
gluten-sensitive enteropathy, only about 20% have intestinal symptoms of celiac
disease (CD). Both
dermatitis herpetiformis and celiac disease are multifactorial disorders in
which genetic and environmental triggering factors play a crucial role, leading
to specific lesions in small bowel and skin, respectively. Both conditions are characterized by the development of IgA
auto antibodies against transglutaminases that, in the case of dermatitis
herpetiformis, IgA antitransglutaminase auto antibodies are deposited in the
dermal papillae which lead to neutrophil infiltration and blister formation. Strong
associations with HLA DQ2 (in 80–90% of patients) and HLA DQ8 (in 10–20% of
patients) have been demonstrated in both diseases. Both the skin and the intestinal disease respond to gluten restriction
and recur with institution of a gluten-containing diet.
Four findings
support the diagnosis of DH:
1. Pruritic papulovesicles or
excoriated papules on extensor surfaces
2. Neutrophilic infiltration of the dermal papillae with vesicle formation at the dermal–epidermal junction
3. Granular deposition of IgA within the dermal papillae of clinically normal-appearing skin adjacent to a lesion (this is essential for the diagnosis and occurs at the site of eventual inflammation)
4. A response of the skin disease,
but not the intestinal disease, to dapsone therapy and worsening
of symptoms with inorganic iodide ingestion.
Although
DH is usually a lifelong condition, the course may wax and wane. A spontaneous
remission may occur in up to 10% of patients, but most clinical remissions are
related to dietary gluten restriction.
Epidemiology
Age
Dermatitis
herpetiform is usually presents in the third decade, although individuals of
any age can be affected.
Sex
DH is commoner in men than women, with a male to female
ratio of 2: 1.
Pathogenesis
The
pathogenesis of DH is based on a number of clinical and laboratory
observations. The key observations that have been integrated into theories of
pathogenesis are:
·
A strong genetic association with
the HLA genotype DQ A1*0501, B1*02 (which encodes HLA-DQ2 heterodimers), in
addition to other unidentified non-HLA genes
·
Some degree of gluten-sensitive
enteropathy on small bowel biopsy in virtually all patients, accompanied by
stimulation of the mucosal immune system
·
Granular IgA deposition within
the papillary dermis of the skin (this is essential for the diagnosis and
occurs at the site of eventual inflammation)
·
Improvement of symptoms with
dapsone therapy and worsening of symptoms with inorganic iodide ingestion.
Genetic predisposition
Specific
HLA genes, which encode molecules that interact with T-cell receptors, are
believed to provide the antigenic specificity that processes the gliadin
antigen in genetically susceptible individuals. This HLA association is the
same for patients with CD and DH. Genes encoding the DQ2 (A1*0501, B1*02)
heterodimer are carried by 90% of CD and DH patients, while genes encoding the
DQ8 (A1*03, B1*03) heterodimer are carried by the remaining DH patients.
Gluten-sensitive enteropathy
On
small bowel biopsy, more than 90% of DH patients have some degree of
gluten-sensitive enteropathy. The bowel abnormality is caused by gluten, a
family of grain proteins present in wheat, rye, and barley, but not oats. Gliadin represents
the alcohol-soluble fraction of glutenis and is believed to be the
antigenic component. The spectrum of intestinal involvement ranges from minimal
infiltration of the lamina propria by lymphocytes (with normal villi), to
minimal atrophy of the jejunum accompanied by
intraepithelial lymphocytic infiltrates, to total villous atrophy of the
small intestine. The enteropathy is often patchy and may require multiple small
bowel samples for diagnosis. Symptomatic
malabsorption occurs in 20% of patients with DH.
Following
ingestion of gluten-containing grains, one of the products of digestion is
gliadin. Once gliadin is absorbed via the lamina propria, glutamine residues
within gliadin are deamidated by tissue transglutaminase (TG2) and covalent
cross-links (isopeptidyl bonds) are formed between lysine residues in TG2 and
glutamines in gliadin. Deamidation by TG2 is thought to be a critical step as
it serves to optimize antigen presentation.
Proposed pathogenesis
of dermatitis herpetiformis and celiac disease

A Dietary wheat, barley or
rye is processed by digestive enzymes into antigenic gliadin peptides, which
are transported intact across the mucosal epithelium. Within the lamina
propria, tissue transglutaminase (TG2): (1) deamidates glutamine residues within
gliadin peptides to glutamic acid; and (2) becomes covalently cross-linked to
gliadin peptides via isopeptidyl bonds (formed between gliadin glutamine and
TG2 lysine residues). B CD4+ T cells in the lamina propria
recognize deamidated gliadin peptides presented by HLA-DQ2 or -DQ8 molecules on
antigen-presenting cells, resulting in the production of Th1 cytokines and
matrix metalloproteinases that cause mucosal epithelial cell damage and tissue
remodeling. In addition, TG2-specific B cells take up TG2–gliadin complexes and
present gliadin peptides to gliadin-specific helper T cells, which stimulate
the B cells to produce IgA anti-TG2. C Over time, in the setting of
continued exposure to gliadin, IgA
directed against TG3 (IgA anti-TG3) forms as a result of epitope spreading in
patients who already have IgA anti-TG2 antibodies and both IgA anti-TG2 and IgA
anti-TG3 circulate in the bloodstream. D When IgA anti-TG3 antibodies
reach the dermis, they complex with TG3 antigens which have been produced by
keratinocytes (epidermal TG) and then have diffused into the dermis. That is,
IgA/TG3 immune complexes are formed locally
within the papillary dermis. This leads to neutrophil chemotaxis (with
formation of neutrophilic abscesses), degranulation of neutrophils releases
proteolytic enzymes that disrupt the lamina lucida, and subepidermal blister
formation.
Deamidated
gliadin peptides bind to the groove of the HLA-DQ2 molecule on dendritic
antigen-presenting cells, and the gliadin antigen is then presented to sensitized
helper T cells in the context of HLA-DQ2 specificity.
These helper T cells can stimulate B cells, with differentiated plasma cells
producing IgA antibodies to multiple antigens,
including gliadin, gliadin cross-linked to TG2, TG2, and epidermal transglutaminase
(TG3). In addition, stimulated natural killer lymphocytes cause crypt
hyperplasia and villous atrophy. Of note, IgA anti-TG2 antibodies have become
the serologic hallmark for CD.
In
the setting of continued exposure to gliadin, epitope spreading is thought to
lead to development of IgA anti-TG3 antibodies in patients who already have IgA
anti-TG2 antibodies; a subgroup of those who develop IgA anti-TG3 antibodies
then develop DH. Epitope spreading is a possible explanation for why DH tends to
present at a later age than symptomatic CD (the latter often manifests in
childhood) and why patients with CD (but not DH) tend to have more severe
intestinal disease than patients with DH. Formation of IgA anti-TG3 antibodies
is thought to require time and continued exposure to gluten and this would be
more likely to occur in patients with less severe, relatively asymptomatic
intestinal involvement. Findings in support of this theory include the presence
of IgA anti-TG2 antibodies in most DH patients and a higher prevalence of IgA
anti-TG3 antibodies in adults than in children with CD (i.e. developing later
in the evolution of the disease).
The
formation of IgA anti-TG3 antibodies also activates circulating neutrophils.
Deposition of these antibodies within the dermal papillae results in the
infiltration of activated neutrophils from the circulation into the dermal
papillae. Degranulation of neutrophils releases proteases which disrupt the
lamina lucida and produce a subepidermal blister.
Since
both the skin disease and the intestinal disease resolve with dietary gluten
restriction and recur with return to a regular diet, it is clear that the
dietary protein gluten is central to the pathogenesis of the cutaneous
eruption. In addition, it is the HLA class II antigen that acts as a gate
through which gluten can reach the inflammatory cells and initiate the
autoimmune process.
Cross-reactivity hypothesis for the onset of dermatitis
herpetiformis in people with celiac disease

Gliadin
proteins in gluten are absorbed by the gut and enter the lamina propria where
they need to be deamidated by tissue transglutanimase (tTG). tTG modifies
gliadin into a more immunogenic peptide. Classical dendritic cells (cDCs)
endocytose the immunogenic peptide and if their pattern recognition receptors
(PRRs) are stimulated by pathogen-associated molecular patterns (PAMPs) or
danger-associated molecular pattern (DAMPs), the danger signal will influence
them to secrete IL-8 (CXCL8) in the lamina propria, recruiting neutrophils.
Neutrophil recruitment results in a very rapid onset of inflammation.
Therefore, co-infection with microbes that carry PAMPs may be necessary for the
initial onset of symptoms in gluten sensitivity, but would not be necessary for
successive encounters with gluten due to the production of memory B and T
cells. In celiac disease, tTG is treated as an autoantigen, especially in
people with certain HLA-DQ2 and HLA-DQ8 alleles and other gene variants that
cause atopy. tTG is up-regulated after gluten absorption. cDCs endocytosetTG-modified
gliadin complexes or modified gliadin alone but they only present gliadin to
CD4+ T cells on pMHC-II complexes. These T cells become activated and polarised
into type I helper T (Th1) cells. Th1 cells against gliadin have been
discovered, but none against tTG. A naive B cell sequesters tTG-modified
gliadin complexes from the surface of cDCs in the lymph nodes (LNs) before they
become endocytosed by the cDCs. The B cell receptor (membrane bound antibody; BCR)
is specific to the tTG portion of the complex. The B cell endocytoses the
complex and presents the modified gliadin to the activated Th1 cell's T cell
receptor (TCR) via pMHC-II. Thus, the B cell presents the foreign peptide
(modified gliadin) but produces antibodies specific for the self-antigen (tTG).
Once the B cell becomes activated, it differentiates into plasma cells that
secrete auto antibodies against tTG, which may be cross-reactive with epidermal
transglutanimase (eTG). Class A antibodies (IgA) deposit in the gut. Some may
bind to the CD89 (FcaRI) receptor on macrophages (M1) via their Fc region
(constant region). This will trigger endocytosis of the tTG-IgA complex,
resulting in the activation of macrophages. Macrophages secrete more IL-8, propagating
the neutrophil-mediated inflammatory response. In dermatitis herpetiformis, the
purportedly cross-reactive auto antibodies may migrate to the skin. IgA
deposits may form if the antibodies cross-react with epidermal transglutanimase
(eTG). Macrophages may be stimulated to secrete IL-8 by the same process as is
seen in the gut, causing neutrophils to accumulate at sites of high eTG
concentrations in the dermal papillae of the skin. Neutrophils produce puss in
the dermal papillae, generating characteristic blisters. IL-31 accumulation at
the blisters may intensify itching sensations. Memory B and T cells may become
activated in the absence of PAMPs and DAMPs during successive encounters with
tTG-modified gliadin complexes or modified gliadin alone, respectively.
Symptoms of dermatitis herpetiformis are often resolved if patients avoid a
gluten-rich diet.
Circulating
antibodies
The first serologic
difference between DH and CD was initially described in 2002, with TG3
identified as the auto antigen in DH. Additional studies have demonstrated that
circulating IgA anti-TG3 antibodies are not only elevated in patients with DH,
but can be assayed and may be helpful in monitoring response to a gluten-free
diet. TG3 is also found to co-localize with IgA in dermal papillae of DH
patients and is enzymatically active in this site. TG3 is expressed in many
tissues of the body, including the epidermis. When IgA anti-TG3 antibodies
reach the dermis, they complex with TG3 antigens which have been produced by keratinocytes
(epidermal TG) and then have diffused into the dermis. In other words, IgA/TG3
immune complexes are formed locally within
the papillary dermis.
In DH skin, IgA-bound deposits of
TG3 are enzymatically active and therefore the TG3 likely plays an important
role in the covalent binding of IgA to connective tissue fibres. Enzymatically
active TG3 also binds to soluble fibrinogen whose subsequent degradation may
play a key pathogenic role.
Dermatitis herpetiformis – DIF

A
Granular IgA deposition along the dermal–epidermal junction of normal-appearing
skin adjacent to a lesion.
B
Granular deposition of epidermal transglutaminase (TG3) within the dermal
papillae, which co-localizes with the IgA.
Granular
IgA deposition
Granular
IgA deposition within dermal papillae is the hallmark of DH. The deposits are
composed of IgA1 antibodies directed against TG3 antigen that has diffused from
the epidermis. Circulating IgA antibodies to TG2 (an endomysial antigen) have
been identified by indirect immunofluorescence microscopy using a monkey
esophagus substrate, and the presence of these antibodies correlates with the
degree of gluten-sensitive enteropathy. IgA anti-TG2 antibodies are not
responsible for the IgA deposition in skin.
Iodide
and Dapsone
Ingestion
of iodide can lead to worsening of DH and topical application of iodide onto
the normal skin of DH patients produces lesions that are histologically
identical to spontaneous lesions. Even in normal subjects, topical iodides may
produce follicular neutrophilic pustules. The mechanism by which iodide
stimulates neutrophil infiltration into the skin is unclear.
Dapsone
is known to have an effect on neutrophil chemotaxis and neutrophil attachment
to IgA in vitro. Although the exact mechanism of its beneficial effect
in DH is unknown, it seems likely that dapsone blocks the neutrophil-mediated
inflammatory process.
Associated Disorders
and Malignancies
A strong association exists between DH and
thyroid disease, particularly Hashimoto’s thyroiditis. The incidence of enteropathy-associated
T-cell small
bowel lymphoma is also increased in patients with
DH and warrants increased surveillance. Of note, adhering to a gluten-free diet
protects against lymphoma in this population. This further supports advising
patients with DH to adhere to a strict gluten-free diet for life.
|
AUTOIMMUNE DISORDERS
ASSOCIATED WITH DERMATITIS HERPETIFORMIS |
|
Common |
|
1.
Autoimmune thyroid disease (Hashimoto’s
thyroiditis) 2.
Insulin-dependent type 1 diabetes mellitus |
|
Uncommon |
|
1.
Pernicious anemia |
|
Rare |
|
1.
Addison’s disease 2.
Autoimmune chronic active hepatitis 3.
Alopecia areata 4.
Myasthenia gravis 5.
Sarcoidosis 6.
Systemic sclerosis (scleroderma) 7.
Sjögren’s syndrome 8.
Systemic lupus erythematosus 9.
Vitiligo |
Clinical Features
History
The principal symptom of patients with dermatitis
herpetiformis is itch. Itching of variable intensity, scratching and
burning sensation immediately preceding the development of lesions are common. Patients report a rash, most typically over the extensor surfaces
of the elbows, knees, buttocks and scalp. Although small bowel
involvement in dermatitis herpetiformis is often asymptomatic in adults, it can
be associated with abdominal pain, bloating,
diarrhea,
iron deficiency and reduced growth rates in children. There may be complaints of other autoimmune diseases
including hypothyroidism.
Presentation
DH has a
symmetric distribution and favors the elbows (90%), knees (30%), extensor
forearms, shoulders, back, buttocks, sacral region, and face. Isolated scalp
involvement is an occasional clinical presentation. The primary lesions are
pleomorphic, with urticarial plaques, papules and vesicles. Grouped or
“herpetiform” papulovesicles with an erythematous base are characteristic.
Because the condition is so pruritic, intact vesicles are rarely seen and the
patient may simply present with excoriations, erosions, crusting and hyper
pigmentation. Even if only hemorrhagic crusts or secondary changes from
scratching are present, the diagnosis should be suspected on the basis of the
distribution of lesions. Lesions heal without scarring. Less common presentations are isolated facial involvement, exclusively
macular lesions, and punctate purpura on the palms and soles. Mucosal
change may occur, and dental abnormalities have been reported, particularly
enamel pits. Interestingly, first‐degree relatives of patient with GSE may also
show enamel defects.
Pattern of distribution

Complications
and co‐morbidities
The principal complications and co‐morbidities of dermatitis
herpetiformis relate to GSE and the associated risk of small bowel lymphoma.
GSE may lead to malabsorption resulting in anaemia, weight loss and
osteoporosis. Rarely, GSE (and consequently dermatitis herpetiformis) may be
associated with neurological changes including ataxia and neuropathy.
Disease
course and prognosis
Dermatitis herpetiformis is a chronic disease that requires
patients to adopt a long‐term gluten‐free diet. Those that are able to do this, and respond, seem
to have excellent long‐term survival and are able to decrease or discontinue
dapsone treatment. Recent data suggest that patients with GSE who do not
respond to a gluten‐free diet do poorly. Whilst the disease is a chronic one,
remission is recognized, and seems to be more common in adult patients over the
age of 40 years.
Investigations
The
diagnosis of dermatitis herpetiformis is made by the presence of characteristic
clinical features, histopathology, direct IF testing and serology.
Histopathology
For routine histology, it is optimal to
capture a small, intact vesicle. If this is not available, an area of erythema
should be biopsied. Areas of erythema will show dermal papillary edema and
neutrophil infiltration associated with a superficial
perivascular lymphocytic infiltrate. Dermal papillae filled with neutrophils
and very few eosinophils, with relative sparing of
the lowermost tips of the intervening rete ridges, is a characteristic finding.
When an intact vesicle is biopsied, a sub epidermal blister containing
predominantly neutrophils is seen. Histopathology of a dermatitis
herpetiformis skin lesion can be evocative, but not diagnostic, and a
non-specific histopathologic picture is often documented. Thus, if DIF is
positive, a biopsy for histology is not necessary.


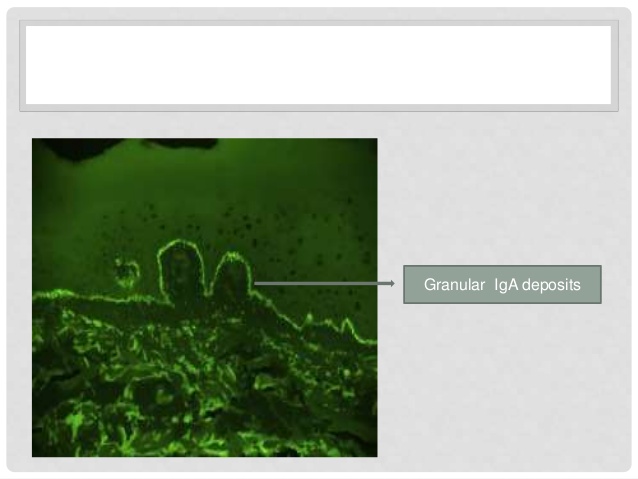
Direct
immunofluorescence (DIF) testing
DIF of uninvolved skin is the gold standard
for the diagnosis of dermatitis herpetiformis. Two different patterns of DIF
are possible: (i) granular deposits in the dermal papillae and (ii) granular
deposits along the basement membrane. Sometimes, a combination of both
patterns, consisting in granular IgA deposition along the basement membrane
with accentuation at the tips of the dermal papillae, may be present.
In patients with DH, dermal IgA
deposits are not uniformly distributed throughout the skin. Notably, IgA
deposits are present in greater amounts near active lesions. The optimal biopsy
site for direct immunofluorescence (DIF) testing is normal-appearing skin
immediately adjacent to a lesion, best on the buttocks. A false-negative DIF can occur if lesional skin is biopsied, since the
inflammatory infiltrate can destroy the IgA. A definitive diagnosis of DH
cannot be made without this diagnostic DIF finding. Granular IgA deposits
localized to the dermal papillae are found in 85% of cases of DH, while
continuous granular deposition of IgA along the basement membrane occurs in 5%
to 10% of cases. A fibrillar pattern of IgA deposition occurs rarely.
The
lack of histologic and immunopathologic confirmation is a source of
misdiagnosis and confusion in DH. Since DH is a lifelong diagnosis with
significant systemic and therapeutic implications, definitive immunopathologic
confirmation of the diagnosis is essential in all cases.
Serologic findings
Serologic tests, and in particular IgA
anti-tTG and EMA testing, have become relatively sensitive and specific tools
for initial detection of gluten-sensitive disease and therefore of dermatitis herpetiformis.
Anti-tTG belongs to the IgA1 subclass and is
directed against tTG antigen. tTG share a 64% homology with epidermal TG, which
represents the target auto antigen of dermatitis herpetiformis, as recently
demonstrated. Anti-tTG are measured using an enzyme-linked immunosorbent assay
(ELISA) and are a useful marker of bowel damage and diet adherence in
dermatitis herpetiformis/celiac disease patients. In dermatitis herpetiformis,
IgA anti-tTG has specificity higher than 90%, and a sensitivity ranging from
47% to 95%.
EMA belong to the IgA1 subclass and are
directed against primate smooth muscle reticular connective tissue. The
endomysium is the connective tissue covering the smooth muscle layers of the esophagus,
stomach and small intestine. The detection of EMA is based on an indirect
immunofluorescence assay on monkey esophagus and it is more time-consuming
and operator-dependent than the one of anti-tTG ELISA testing. EMA testing has
shown specificity close to 100%, and a sensitivity ranging from 52% to 100% for
the diagnosis of dermatitis herpetiformis. As for anti-tTG, EMA are usually
absent in patients on GFD and thus represent a useful diet-compliance marker in
celiac disease/dermatitis herpetiformis subjects.
Other auto antibodies, such as antigliadin
antibodies and antireticulin antibodies, are no longer considered a sensitive
and specific marker of dermatitis herpetiformis. Their detection predates the
previously described serologic tests, but the diagnostic performance is not
advantageous compared with that of IgA anti-tTG and EMA.
Interestingly, very recently, it has been
shown that tests detecting both antibody isotypes (IgA and IgG) against
deamidated synthetic gliadin-derived peptides may be considered as the most
reliable serologic tool in order to identify gluten sensitivity in dermatitis
herpetiformis patients. However, further studies are required to confirm such
findings.
Other tests to be performed in dermatitis herpetiformis patients
Although unnecessary for dermatitis
herpetiformis diagnosis, other tests such as small bowel biopsy, HLA testing,
screening for autoimmune diseases and associated conditions and evaluation of
malabsorption should be performed in dermatitis herpetiformis patients to have
an accurate global assessment of the patient.
Steatorrhea in 20 to 30%) and abnormal
D-xylose absorption in 10 to 73% is found. Anemia is secondary to iron or
folate deficiency. Endoscopy of small bowel: blunting and flattening of the villi
(80 to 90%) in the small bowel as in celiac disease. Lesions are focal;
verification is by small-bowel biopsy.
Small bowel biopsy
Since dermatitis herpetiformis can be
considered the cutaneous counterpart of celiac disease, a proven diagnosis of
dermatitis herpetiformis in a patient should be used as diagnostic tool for
bowel damage recognition. Accordingly, small bowel biopsy would be unnecessary
in dermatitis herpetiformis patients, and diet adherence would be monitored by
serological testing and skin lesions observation (as it is known, dermatitis
herpetiformis lesions usually recur within few days after gluten ingestion).
Indeed, very recently, it has been suggested that small bowel biopsy is no
longer regarded as mandatory for the diagnosis of celiac disease at least in a
subgroup of patients.

HLA haplotypes testing
As in celiac disease, virtually all patients
with dermatitis herpetiformis carry either HLA DQ2 or HLA DQ8 haplotypes. Thus,
the presence of these alleles provides a sensitivity of close to 100% for
dermatitis herpetiformis and a very high negative predictive value for the
disease (i.e. if individuals lack the relevant disease-associated alleles,
celiac disease is virtually excluded). HLA testing for the relevant DQ alleles
can be a very useful adjunct in an exclusionary sense when the diagnosis based
on other test results is not clear. In contrast, given the marked prevalence of
the celiac disease-associated HLA class II alleles in the general population,
the specificity of these alleles for the disease is poor.
Screening for autoimmune diseases and associated conditions
Considering the increased incidence of
immunomediated diseases and associated conditions, several screening tests
should be performed in patients with dermatitis herpetiformis. Nonspecific
antibodies, such as antithyroid peroxidase (in almost 20% of patients),
antigastric parietal cells (in 10–25% of patients), antinuclear and anti-Ro/SSA
antibodies, should be tested in celiac disease/dermatitis herpetiformis
patients. The presence of such antibodies correlates with autoimmune
predisposition of celiac disease/dermatitis herpetiformis patients.
Furthermore, testing for thyroid disease (TSH, T3 and T4)27 and for diabetes
(glucose) should be performed.
Finally, although, a very recent work has
shown lack of increased risk of lymphoma in people with dermatitis
herpetiformis in comparison to the general population, it is recommended to pay
clinical attention to the potential development of intestinal or
extra intestinal lymphoma.
Screening first-degree relatives for celiac disease
Since the incidence of celiac disease is
higher in dermatitis herpetiformis/celiac disease patients’ relatives, a
screening for celiac disease in first degree relatives of the patients should
be done. However, although the utility of testing for celiac disease in
symptomatic first-degree relatives is clear, there is currently little evidence
to support screening in asymptomatic first-degree relatives.

DGP = IgA and IgG anti-deamidated
synthetic Giadin derived peptides (DGP), EMA= anti-endomysial antibodies
IgA anti-tTG and anti-endomysial
antibodies (EMA) can be monitored over time to assess compliance with a
gluten-free diet. Because the anti-endomysial antibody assay is based upon
analysis of indirect immunofluorescence, it is more expensive and not as
readily available as the IgA anti-tTG antibody assay; thus, the recommendation
that the latter assay be performed first. Ab, antibody; DIF, direct
immunofluorescence; tTG, tissue transglutaminase.
|
CHARACTERISTICS
THAT DIFFERENTIATE DH, LABD AND BP |
|||
|
DH |
LABD |
BP |
|
|
Cutaneous
lesion |
Grouped
papules and small vesicles, often excoriated |
Small
vesicles and/or large bullae |
Large
tense bullae |
|
Distribution |
Extensor
surfaces, symmetrical |
Similar
to DH or BP |
Trunk,
extremities, occasionally mucosal surfaces |
|
Histology |
Sub epidermal
bullae with neutrophilic infiltrate |
Sub epidermal
bullae with neutrophilic infiltrate |
Sub epidermal
bullae with eosinophilic infiltrate |
|
Direct
IF |
Granular
IgA in dermal papillae |
Linear
IgA at BMZ, possibly also IgG |
Linear
IgG and C3 at BMZ |
|
Site to
biopsy for direct IF |
Adjacent
normal-appearing skin |
Perilesional |
Perilesional |
|
Indirect
IF |
Negative |
Linear
IgA at BMZ (70%) |
Linear
IgG at BMZ (70%) |
|
Enteropathy |
>90% |
Rare |
None |
|
HLA-DQ2 |
>90% |
30% |
Normal
(20%) |
|
Dapsone
responsiveness |
Excellent |
Good,
may also require systemic corticosteroids |
Minimal
to moderate |
Diagnosis and
differential diagnosis
Grouped papulovesicles at
predilection sites accompanied by severe pruritus are highly suggestive. Biopsy
usually diagnostic, but IgA deposits in perilesional skin detected by IF are
the best confirming evidence.
Differential diagnosis are
allergic contact dermatitis, atopic dermatitis, scabies, neurotic excoriations,
papular urticaria, and bullous autoimmune disease
Treatment
The
treatment of DH includes a gluten-free diet (GFD) and dapsone, as well as a
combination of the two therapies. Because several months of gluten-free diet
therapy are needed for a response, most patients with dermatitis herpetiformis
require concurrent pharmacological intervention to control their disease in the
short to medium term. Dapsone and related sulphonamide drugs have proven highly
effective.
GFD
The cornerstone of long‐term
dermatitis herpetiformis management is strict adherence to a gluten‐free
diet (which includes corn, rice and oats).
A GFD is the treatment of choice for patients with celiac disease/dermatitis
herpetiformis since both the enteropathy and the cutaneous rash depend on
gluten. GFD alleviates gastrointestinal symptoms much more rapidly than the
rash: it takes an average of 2 years of GFD for complete elimination of the
cutaneous lesions, which invariably recurs within 12 weeks after the
reintroduction of gluten. The following advantages observed in dermatitis
herpetiformis patients on a long-term GFD are reduced or no need for
medication, resolution of enteropathy and the correlated malabsorption of
essential nutrients (and therefore prevention of alimentary deficiency of iron,
vitamin B12 and folate), a general feeling of well-being, protective effects
against development of intestinal lymphoma.
IgA antibodies may disappear from the dermal-epidermal junction after
many years of a strict GFD. On reintroduction of gluten, IgA deposits reappear
in the skin and skin disease return. In addition, minor fluctuations in disease
severity are most likely related to oral gluten intake. The gluten-free diet is
inconvenient and unacceptable to some patients.
The cereal species whose proteins are toxic
to patients with celiac disease/dermatitis herpetiformis are grasses of the
tribe Triticeae, which includes wheat, rye and barley. Although in the past the basis of GFD was the
avoidance of all gluten-containing cereals, including wheat, barley, rye, and
oats (mnemonic BROW), recently, some authors have demonstrated that oats
belonging to the Avenae tribe can be safely consumed by celiac
disease/dermatitis herpetiformis patients. However, only oats known to be pure
and not contaminated in any way with wheat, barley or rye (which is the case of
the majority of commercially available oats) can be safely consumed.
Although
GFD offers many benefits in the management of dermatitis herpetiformis, it is
not easy to realize by many dermatitis herpetiformis patients. A GFD requires
scrupulous monitoring of all ingested foods; it is time-consuming and socially
restricting. Strict adherence to a GFD requires extensive knowledge of foods
and diet, thus consultation with a dietician and involvement in dermatitis
herpetiformis support groups are strongly encouraged. In general, patients
following a GFD are advised to read carefully all food labels and to avoid
products with unfamiliar ingredients. Many food ingredients (i.e. additives,
cereal grains, natural and artificial colorings, emulsifiers, excipients,
artificial flavorings, malts, hydrolyzed plant and vegetable proteins,
monosodium glutamate, preservatives, natural and modified food starches,
vegetable gum, vinegar) may be derivatives of gluten-containing products.
Dapsone
Dapsone
represents a valid therapeutic option for dermatitis herpetiformis patients
during the 1- to 2-year period until the GFD is effective; dapsone does
effectively decrease pruritus and inflammatory lesions. The pruritus of DH is relieved within 48–72
hours of instituting dapsone. The lesions abruptly recur within 24–48 hours of
discontinuation of therapy. Unfortunately, dapsone has no effect on the
intestinal pathology.
Dapsone
is begun after screening for glucose-6-phosphate dehydrogenase (G6PD)
deficiency, with initial dosages of 25–50 mg in adults and 0.5 mg/kg in
children. Initiation of therapy with higher doses may precipitate severe
hemolysis and cardiac decompensation in susceptible individuals. The average
maintenance dose in adults on a normal diet is 100 mg daily. The half-life
ranges from 12 to 24 hours, so divided doses are seldom of benefit. The daily
dose can be regulated on a weekly basis to optimize control. One to two new
lesions per week should be expected on the optimal dose. Higher doses simply
increase toxicity with little benefit.
Outbreaks
of facial and scalp lesions while on otherwise adequate treatment can occur,
but are not common. Facial disease may prove refractory to dapsone therapy.
Breaking the vesicles followed by application of a potent corticosteroid gel
may be helpful.
The
mechanism of action of dapsone in dermatitis herpetiformis is through its
effects on neutrophil function and recruitment.
Although
there are many side effects of dapsone, the drug is well tolerated for years in
more than 90% of patients. In particular, the commonest side-effect of dapsone
is hemolysis and patients should be seen within 2 weeks after starting the
drug as hemolysis may be acute in some individuals. Hemolysis occurs in
virtually every patient on dapsone therapy, since sulfones produce an oxidant
stress on aging red blood cells. In patients with G6PD deficiency, dapsone may
produce severe hemolysis. Although most patients have evidence of drug-induced
hemolysis, a compensated haemolytic anaemia does develop. Drug-induced hemolysis
can be confirmed and followed by a reticulocyte count, which should show
increased erythropoiesis. Of note, dapsone is secreted in breast milk and may
cause hemolytic anemia in breastfed infants. In the setting of a persistent
severe anemia, a search for contributing causes, such as iron, vitamin B12
or folate deficiencies or hereditary spherocytosis, should be performed.
Methemoglobin
is present in the blood of most patients taking 100 mg of dapsone daily.
Although the amount of methemoglobin usually does not exceed 5%, there are
patients who have maintained levels between 10% and 15%. Methemoglobinemia in
the absence of cardiopulmonary symptoms does not require alteration of dapsone
dose. Patients should be warned that arterial
desaturation may be noted by pulse oximetry, even with relatively low levels of
methemoglobinemia.
Fatal
agranulocytosis has developed in patients with DH treated with dapsone. This
drug-induced agranulocytosis usually occurs after 2–12 weeks of continuous
dapsone treatment. A hypersensitivity reaction involving the formation of
leukocyte agglutinins seems to be the underlying mechanism. Re-administration
of dapsone then causes leukopenia within hours. A simple measure is to warn the
patient to discontinue the drug and report immediately if fever, a sore throat,
or other signs of infection develop.
Dapsone
hypersensitivity syndrome is a rare, but potentially severe, reaction,
characterized by fever, a cutaneous eruption and internal organ involvement, which
develops in about 5% of dermatitis herpetiformis patients 2–6 weeks after the
beginning of treatment. The cutaneous manifestations vary from a morbilliform
eruption to exfoliative dermatitis, while the systemic manifestations include,
lymphadenopathy, hepatitis, an elevated ESR, leukocytosis, and, rarely,
eosinophilia. Patients should be educated about this syndrome and instructed to
discontinue therapy and notify their medical provider if any signs or symptoms
of the dapsone hypersensitivity syndrome develop.
Peripheral
neuropathy induced by dapsone may occur as early as during the first 4 months
of therapy. Indeed, neuropathic signs can develop within the first few weeks of
therapy. The neuropathy was initially reported as a pure motor neuropathy
(involving primarily distal extremity muscles); however, pure motor, pure sensory
and combined motor and sensory neuropathies have subsequently been reported.
Relatively high daily doses of dapsone (200–500 mg) and high cumulative doses
in the range of 25 to 500 g have been implicated.
Dapsone
should always be used in combination with a gluten‐free diet.
With time, it may be possible to decrease and potentially withdraw dapsone
without relapse, as long as the patient is able to adhere to the diet.
Dapsone
therapy monitoring includes a baseline complete blood count (CBC) and liver
function tests, then weekly CBCs for the first month, monthly CBCs for the next
5 months, and semi-annual CBCs thereafter while the patient remains on therapy.
Liver function tests should be repeated at 6 months and annually thereafter.
Some clinicians measure baseline G6PD activity in all patients, while others
focus on those of African, Asian or southern Mediterranean ancestry.
Dapsone adverse effects
1 Toxic/Pharmacologic
·
Methemoglobinemia
·
Hemolytic anemia
2 Idiosyncratic/Allergic [Dapsone
hypersensitivity syndrome]
·
General malaise
·
Exanthematous eruption, Stevens–Johnson syndrome/Toxic Epidermal
Necrolysis
·
Photosensitivity
·
Neurological effects:
peripheral neuropathy, optic nerve atrophy, psychosis, headache, nervousness,
lethargy, depression
·
Nephropathy: nephritis,
renal failure
·
Hypothyroidism
·
Gastro-intestinal effects:
nausea, vomiting, gastro-intestinal upset
The main adverse reactions to dapsone,
classified as toxic and idiosyncratic. Such adverse effects are usually dose
dependent and more common in patients with comorbidity (anemia,
cardiopulmonary disease, glucose-6- phosphate-dehydrogenase deficiency).
Sulfasalazine and sulphamethoxypyridazine
Sulfasalazine and sulphamethoxypyridazine
might provide an effective alternative to dapsone especially when it fails to
control the disease or the therapy is complicated by adverse events. The
suggested dosages are of 1–2 g/day for sulfasalazine and of 0.25–1.5 g/day for
sulphamethoxypyridazine. Both drugs
share common adverse effects, including hypersensitivity reactions, hemolytic
anemia, proteinuria and crystalluria; thus, a full blood count with differential
and urine microscopy with urinalysis should carried out prior to starting
treatment and monthly for the first 3 months of therapy, and thereafter once
every 6 months. However, the most common adverse effects are nausea, anorexia
and vomiting, which can be prevented by prescribing the enteric-coated forms of
the drugs. Adequate fluid intake and alkalinization of the urine minimizes the
risk of nephrolithiasis.
Corticosteroids
While orally administered corticosteroids
give poor results, application of potent or very potent topical steroids (especially
clobetasol propionate) can be useful in the short term to decrease pruritus
and itching.
Anti-histamines
Although their efficacy is not very high in
the treatment of dermatitis herpetiformis, third-generation antihistamines with
specific activity on eosinophilic granulocytes, classified as a third-level
therapeutic option, may also be used to control pruritus and itching.

Dermatitis herpetiformis monitoring
Follow-up is necessary to confirm the
diagnosis by an objective response to a GFD and to detect and manage
non-compliance. Patients with dermatitis herpetiformis/celiac disease should be
evaluated at regular intervals (i.e. 6 months after diagnosis and then yearly)
by a health care team including a physician and a dietician. These visits can
be used to assess, by history, a patient’s compliance with a GFD, to reinforce
the importance of such compliance and to evaluate the possible development of
intestinal malabsorption and/or dermatitis herpetiformis–associated
conditions. In general, monitoring
adherence to a GFD with serological investigations (i.e. anti-tTG or EMA) is
sensitive for major but not for minor transient dietary indiscretions. Table 1
lists the main targets in monitoring. Follow-up examinations recommended for
celiac disease/dermatitis herpetiformis patients are summarized in Table 2.
Table 1
Indications for monitoring
·
GFD adherence
·
Possible development of an
autoimmune associated disease (despite GFD adherence)
·
Metabolic alterations
(dyslipidemia, non-alcholic steatohepatitis)
·
Possible development of
neoplastic (lymphoma) or non–neoplastic (refractory celiac disease, ulcerative
jejunoileitis, collagenosic sprue) complications
Table 2
Item list for routine check-ups
·
Physical examination
·
Dietician counselling
·
Serological laboratory tests
(haemochrome, malabsorption evaluation: sideremia and ferritin levels, mean
corpuscular volume, glucose, thyroid hormones)
·
Immunological and autoimmune
markers (dermatitis herpetiformis– specific and non-specific auto antibodies)
Management algorithm for dermatitis herpetiformis
First line
·
Gluten‐free
diet
·
Dapsone
25–150 mg daily
·
Potent
topical steroid
Second line
·
Sulphamethoxypyridazine
0.5–1.5 g daily (with gluten‐free diet)
Third line
·
Sulphapyridine
250–750 mg daily
Or
·
Sulphasalazine
1–2 g daily (with gluten‐free diet)