Urticaria
Salient
features
·
Urticaria
is defined as a skin disorder characterized by local transient skin or mucosal
edema (wheal) and an area of redness (erythema) that typically accompanies
itchy sensations and diminishes within 1 day.
·
Symptoms
may occur either spontaneously (spontaneous or idiopathic urticaria) or in
response to specific stimuli, such as physical stimuli or sweating (the
increase of body core temperature).
·
Mast
cells and their histamine being released either spontaneously or in response to
various stimuli play a crucial role in the pathogenicity of urticaria.
·
Spontaneous
or idiopathic urticaria is the subtype of urticaria that most patients
experience.
·
Autoantibodies
against immunoglobulin (Ig) E or the high-affinity IgE receptor (FcεRI) that
activate mast cells and basophils and induce histamine release may be detected
in up to half of patients with chronic spontaneous or idiopathic urticaria
(type II autoimmunity).
·
There are several recognizable clinical patterns of urticaria
and different causes. The latter include allergy, autoimmunity, drugs, dietary
pseudo allergens, and infections. Many cases of spontaneous urticaria remain
unexplained (“idiopathic”) even after an extensive evaluation.
·
A
certain population of patients may develop angioedema mediated by bradykinin
rather than histamine.
·
Diagnosis is based primarily on the history and clinical
examination. Determination of the etiology or triggers, as well as exclusion of
other diagnoses, may require further investigations, including blood tests,
physical and dietary challenges, skin tests, and skin biopsy
·
Nonsedative
second-generation antihistamines are the mainstay of pharmaceutical therapy.
·
Omalizumab,
anti-IgE antibody, or immunosuppressive medications may be taken for the
treatment of urticaria and angioedema that is refractory to antihistamines even
at high doses.
Introduction
The urticarias are
characterized by short-lived swellings of the skin and mucosa due to plasma
leakage. The term ‘urticaria’ is a disease that may present with weals, angioedema
or both. Weals and angioedema often occur together and are similar processes
resulting from superficial and deep swellings, respectively.
The
triple
response of Lewis is a cutaneous response that occurs from firm
stroking of the skin, which
produces an initial red line, followed by a flare around that line, and then
finally a wheal. The
triple response of Lewis is due to the release of histamine and
consisting of:
1.
Red spot:
due to capillary dilatation
2.
Flare:
redness in the surrounding area due to arteriolar dilatation mediated by axon
reflex.
3.
Wheal:
due to exudation of fluid from capillaries and venules due to increased
vasopermeability.

Wheals are
swellings of the superficial dermis
due to edema of the papillary body
and are itchy,
well-demarcated, non-pitting, raised swellings of the skin, pink or pale in the center, often with a surrounding red flare
initially. They occur anywhere on the body, any numbers, sizes, and shapes and individual
lesions resolve
spontaneously within 24 h, leaving the skin with a normal appearance.
Angioedema swellings occur deeper in the dermis and in the
subcutaneous or submucosal tissue. Angioedema usually affects the most distensible
tissues, such as the eyelids, lips, ears lobes and external genitalia, or the
mucous membranes of the mouth, tongue, pharynx
or larynx or a portion of an extremity such as hands or feet. The areas of involvement tend to be normal or faint pink in
color, painful rather than itchy (fewer type C nerve endings in the deeper
cutaneous levels), larger and less well defined than wheals, and usually lasting for up to 3 days. Depending on the location (tongue, throat,
glottis), there may be an acute risk of suffocation.
Thus
wheal and angioedema are thus the same edematous process but involving
different levels of the cutaneous vascular plexus: papillary and deep.
Anaphylaxis is an acute, severe,
life-threatening, systemic reaction often involving
the skin due to mast cell mediator release that may be allergic or non‐allergic. It consists of a
combination of symptoms and signs, including diffuse erythema, pruritus,
urticaria and angioedema, hypotension and difficulty in breathing.
Epidemiology
Incidence
and prevalence
An estimate of
the lifetime occurrence of urticaria is likely to be in the range of 1–5% in
the general population.
Age
Urticaria may occur at any age.
Acute spontaneous urticaria often presents in childhood but the peak incidence
of chronic spontaneous urticaria is in the fourth to fifth decades.
Sex
Women outnumber men by 2: 1 with
chronic spontaneous urticaria but there is no sex difference in either acute
spontaneous urticaria or the inducible urticarias.

Pathophysiology
Mast cells settle in connective tissues and usually do not
circulate in the blood stream.
Basophils are the smallest circulating granulocytes. They arise
in the bone marrow, and following maturation and differentiation, are released
into the blood circulation. If they are adequately stimulated they may settle
in the tissues.
Both mast cells and basophils
contain special cytoplasmic granules which store preformed mediators
of inflammation. The extracellular release of the mediators is known as degranulation.
Two types of mast cells have been found by
immunohistochemical analyses. The MCTC type contains
neutral proteases tryptase and chymase and predominates in normal skin and
intestinal submucosa, whereas the MCT type contains
only tryptase, and predominates in normal intestinal mucosa and lung alveolar
wall. Nearly equivalent concentrations of each type are found in nasal mucosa. Both
types, however, express high-affinity IgE receptors (FcϵRI) and are therefore
capable of participating in IgE-dependent allergic reactions.
Mast cell activation
The mast cell is the primary
effector cell of urticaria. Mast cells
are widely distributed throughout the body but vary in their phenotype and
response to stimulation. This may explain why systemic features, such as those
seen in anaphylaxis, do not accompany the activation of cutaneous mast cells in
urticaria.
Mast cell may be activated by immunological
stimulation with activation of the high-affinity IgE receptor (FcεRI) or by
non-immunological IgE-independent stimulation (e.g., by direct histamine
liberation of opiates or neurotransmitters such as substance P, physicochemical
stimuli, by pseudo allergens such as acetylsalicylic acid, infections via possible
complement activation, immune complexes, pathogen-specific IgG or IgE,
bacterial toxins).
Immunological (Allergic)
Cross-linking
of two or more adjacent α-subunits of high-affinity IgE receptors
(FcεRIα) on the mast
cell membrane will initiate a chain of calcium- and energy-dependent steps
leading to fusion of storage granules with the cell membrane and
externalization of their contents. This is known as degranulation. Classic
immediate hypersensitivity reactions involve binding of receptor-bound specific IgE by
allergen. There are also several recognized immunologic
degranulating stimuli that act through the IgE receptor, such as anti-IgE and
anti-FcεRI auto antibodies. However, not all auto
antibodies with these specificities are functional, i.e. capable of releasing
histamine from mast cells or basophils in vitro.
Non-immunological (Non- allergic)
Drugs, including opiates such as morphine and codeine, vancomycin and
polymyxin; some radiocontrast media; and some foods, such as strawberries; C5a anaphylatoxin, stem cell factor and neuropeptides (e.g.
substance P), can cause mast cell degranulation by binding specific receptors,
independent of the FcϵRI.

|
Immunological and non‐immunological mast cell degranulation stimuli. The mast
cell responds with degranulation to non‐immunological as well as immunological stimuli in vitro. It is often difficult, if
not impossible, to know the exact cause of degranulation in vivo. PAMPs, pathogen‐associated
molecular patterns; SCF, stem cell factor; SP, substance P. |
|

Proinflammatory mediators
There are two categories of pro inflammatory mediators in
mast cells and basophils.
Preformed mediators, stored in secretory granules and secreted upon cell
activation, include a biogenic amine, typically histamine, proteoglycans,
either heparin, chondroitin sulphates or both, and a spectrum of neutral
proteases.
Newly generated mediators, often absent in the resting mast cells, are typically
produced during IgE-mediated activation and consist of arachidonic acid
metabolites, principally leukotrienes and prostaglandin and platelet activating
factor. Prostaglandins and leukotrienes are synthesized from arachidonic acid
derived from cell membrane phospholipids. The most important pro inflammatory
eicosanoids are prostaglandin (PG) D2 and the leukotrienes (LT) C4,
D4 and E4 (slow releasing substance of anaphylaxis). PGE2
has inhibitory effects on immunologic mast cell degranulation and may therefore
have a protective role in urticaria.
Mast cells can produce a wide variety of cytokines. Newly
synthesized cytokines are IL-2, IL-3, TNFα, IL-4, IL-5, IL-6, IL-8, and IL-13.
Some cytokines are pre-made and stored in granules for immediate release upon
activation (IL-4, TNFα, and GM-CSF).
Both preformed and newly synthesized pro inflammatory
mediators are released from mast cells upon activation.
Blood Vessels
Histamine and other proinflammatory mediators released on
degranulation bind receptors on post capillary venules in the skin, leading to
vasodilation and increased permeability to large plasma proteins, including
albumin and immunoglobulins. Furthermore, histamine, TNF-α, and IL-8 up-regulate
the expression of adhesion molecules on endothelial cells, thereby promoting
the migration of circulating inflammatory cells from the blood into the
urticarial lesion.
Blood
Autoantibodies
Functional IgG auto antibodies
against IgE or the high‐affinity
IgE receptor that release histamine (and other mediators) from mast cells and
basophils have been detected in the serum of 25–30% of patients with chronic
spontaneous urticaria. Binding of the auto antibodies to mast cells and
basophils may initiate complement activation with the generation of C5a
anaphylatoxin, which in turn facilitates or augments degranulation.
Leukocytes
Blood basophils are reduced in
number in chronic ordinary urticaria patients. Basophils are recruited into
urticarial wheals after weal initiation and may contribute to the persistence
of wheals by releasing histamine and other mediators.
Eosinophil, neutrophil and lymphocyte numbers are normal in
the peripheral blood, but these cells are often present in wheals. Eosinophils
may contribute to the persistence of wheals by generating LTC4, LTD4
and LTE4 and by releasing toxic granule proteins, including major
basic protein (MBP), which can release histamine from basophils. The
function of neutrophils and lymphocytes in urticaria has not been elucidated.
Neuropeptides
Some mast cells are positioned close to nerve endings.
Histamine can stimulate sensory afferent nerves to release substance P, responsible
for the neurogenic axon flare.
Mechanisms
of Urticaria Formation
Mast cell-dependent urticaria
Cross-linking of the Fab portion of specific IgE on mast cells by
percutaneous or circulating allergen undoubtedly accounts for some cases of
acute or episodic urticaria, but this is probably never the cause of chronic
spontaneous urticaria. Examples of the former would be contact urticaria from
natural rubber latex and acute urticaria from foods, including nuts, fish, and
fruit. However, the majority of acute urticaria cases do not relate to allergen
exposure. Binding of pathogen‐associated molecular patterns
(PAMPs) on microbes to toll‐like
receptors on mast cells may be relevant to the pathogenesis of acute urticaria,
which is more often linked to acute viral or bacterial infections than any
other etiology but experimental proof for this is lacking.
It is often difficult to know the exact pathogenesis of individual
cases of urticaria, and many cases remain idiopathic after evaluation.
IgE has
been implicated in the pathogenesis of symptomatic dermographism, cold
urticaria and solar urticaria, but the mechanism by which it renders skin mast
cells more sensitive to physical stimulation is not certain. It is proposed
that the physical stimulus in these patients induces a neoantigen that reacts
with specific IgE antibody bound to mast cells. An additional mechanism, such
as neuropeptide release, could initiate or potentiate mast cell activation.
Using electron microscopy, localized platelet clumping has been demonstrated in
cold urticaria, and the release of platelet mediators, including
platelet-activating factor (PAF) and platelet factor 4/CXCL4, could contribute
to wheal formation.
Cholinergic
urticaria develops in response to stimulation of cholinergic sympathetic
innervation of the sweat glands. How release of acetylcholine from the nerve
endings leads to mast cell activation and histamine release is unknown. An
allergy to sweat has been demonstrated by one group of investigators. It has
been proposed that pressure-induced wheals may be due to a late-phase reaction,
but an antigen has never been identified.
The
initiating event for spontaneous urticaria wheals is unclear but may involve
plasma leakage due to local factors such as heat or pressure, which allows the
extravasation of auto antibodies or IgE-directed antigens that then activate
the IgE receptor, thus leading to mast cell degranulation and a subsequent
urticarial response. As functional auto antibodies cannot be detected in ~70%
of chronic urticaria sera by currently available tests, other mechanisms may
operate in “non-autoantibody” urticaria, which, nevertheless, has a similar
clinical presentation. Increased plasma levels of prothrombin fragment 1 + 2 (F
1 + 2) and D-dimer (a measure of fibrinolysis) have been demonstrated in
CSU and relate to disease severity, but the contribution of coagulation
abnormalities to the pathogenesis remains unclear.
A
popular hypothesis is that dietary food additives and natural salicylates as
well as nonsteroidal anti-inflammatory drugs (NSAIDs) may cause urticaria via
the diversion of arachidonic acid metabolism from prostaglandin to leukotriene
formation. The whealing is caused by direct action of LTC4, LTD4, and LTE4 on small blood vessels. There is some evidence
that PGE2 can have inhibitory effects on immunologic
mast cell degranulation, so a reduction in their formation may facilitate the
latter. Aspirin can aggravate urticaria
in up to 30% of patients with chronic disease, and so avoidance of dietary
pseudo allergen give encouraging results. Aspirin allergy as a cause of urticaria is much less common, and the
proportion of patients with urticaria due solely to pseudo allergens is probably
low.
Understanding
“idiopathic” urticaria remains an important challenge. From a clinical
perspective, it should be regarded as a multifactorial problem, and searching
for aggravating factors is just as important as looking for causes.
Mast cell-independent urticaria
There
are several recognized circumstances where angioedema or wheals are due to
mechanisms that do not involve mast cells. These need special consideration because
their management and prognosis are different. For example, prostaglandins are
involved in the pathogenesis of some patterns of non-immunologic contact
urticaria (e.g. to benzoic acid), and the latter can be suppressed by NSAIDs.
In the cryopyrin-associated periodic syndromes (CAPS), patients often develop
urticarial lesions. Systemic symptoms, such as fever, help to distinguish
patients with autoinflammatory syndromes from those with CSU. The significant
improvement that results from the administration of anakinra, an IL-1 receptor antagonist, rilonacept, a fusion protein that contains the
extracellular domain of the IL-1 receptor and functions as an IL-1 trap,
or canakinumab, a human anti-IL-1β monoclonal
antibody, points to the role of the cryopyrin inflammasome and its production
of IL-1β.
Mechanisms of urticaria formation
The pathomechanism of weals
and angioedema result from transient vasopermeability (due
to a local increase in permeability of capillaries and venules and plasma
leakage leading to wheals/edema) and
vasodilatation of the dermal and subcutaneous vasculature (erythema), axon reflex (erythema halo) as well as
stimulation of sensory nerves (itching) following the release of
preformed and newly synthesized mast cell mediators. In longer lasting lesions accumulation of immune cells (infiltrate) also
occurs. Histamine is the major preformed mediator in most patients. The
clinical improvement on treatment with H1 antihistamines underlines the role of
mast cell-derived histamine as a major mediator in urticarias. Activation of H1
receptors in the skin induces itching, flare, erythema and wealing whereas activation
of H2 receptors contributes to erythema and wealing, but not itch or flare.
The key to diagnosis and therapy is the understanding of
the trigger of mast cell activation with degranulation and release of
mediators.

Possible causes of urticaria
|
Category |
Example |
|
Allergic (IgE-mediated) |
Food Medication
(β-lactam antibiotics) Aeroallergens Contact
allergens Other proteins |
|
Pseudo allergic (not IgE-mediated) |
Acetylsalicylic acid (aspirin) Other
nonsteroidal anti-inflammatory drugs (NSAIDs) Food
additives (additives) Radio contrast media |
|
Physical |
Shear forces Vertical
pressure Cold Heat Ultraviolet light, visible light |
|
Infections |
Bacterial infection (Helicobacter pylori, Streptococcus) Viral
infection (flu-like infection) Parasites (e.g., blastocystis hominis) |
|
Autoreactive/autoimmune |
Hashimoto’s thyroiditis, Graves’
disease |
|
Paraneoplastic |
Lymphoproliferative disease, acute
myeloid leukemia, solid tumors |
|
Psychic |
Stress Traumatic
stress Depression |
|
Increased body temperature |
Physical exertion Emotional
stress Hot bath or hot shower |
|
Idiopathic |
|
Estimated frequency of different
etiologies of selected urticaria forms in each of 100 affected adultsa
|
|
Infections |
Allergic |
Pseudoallergic,
not IgE-mediated |
Autoreactive |
Unknown |
|
Acute spontaneous urticaria |
50 |
10 |
25 |
0 |
20 |
|
Chronic spontaneous urticaria |
50 |
<1 |
20 |
35 |
20 |
|
Cold urticaria |
10 |
0 |
0 |
0 |
90b |
|
Contact urticaria |
0 |
60 |
40 |
0 |
0 |
|
Exercise-induced urticaria |
0 |
30 |
0 |
0 |
70b |
aCombinations are possible
bTrigger is known, but not the etiology
Mast cells are found in the vicinity of
blood vessels, skin adnexae, and nerves. They can be degranulated by immunological
stimulation with activation of the high-affinity IgE receptor (FcεRI) or by
non-immunological IgE-independent stimulation (e.g., by direct histamine
liberation of opiates or neurotransmitters such as substance P, physicochemical
stimuli, by pseudo allergens such as acetylsalicylic acid, infections via
possible complement activation, immune complexes, pathogen-specific IgG or IgE,
bacterial toxins). The activation of FcεRI can be achieved by cross-linking the
specific IgE antibodies bound to the receptor (allergic hypersensitivity
reaction of immediate type, type I according to Gell and Coombs) or
by autoantibodies that bind directly to the receptor or to IgE itself
(autoreactive).
The latter has so far only been shown for
chronic spontaneous urticaria. In about one-third of patients with chronic
urticaria, IgG auto antibodies against IgE or the high-affinity IgE receptor
(anti-FcεRI) can be detected, some of which have functional activity on
basophilic granulocytes and/or mast cells (induction of histamine release,
sulfide-leukotriene production, surface expression of activation markers such
as CD63, CD203c). In recent years IgE auto antibodies against thyroid
peroxidase, interleukin-24, and staphylococcal exotoxins were detected in some
patients with chronic spontaneous urticaria. In addition, the intradermal
testing of autologous serum is positive in a subgroup (autologous serum test),
but this does not correlate with the presence of the auto antibodies mentioned
above.
After activation, the cutaneous mast cells
secrete preformed (histamine, heparin, proteases) as well as newly formed
(prostaglandins, leukotrienes) mediators and cytokines (tumor necrosis factor
α, interleukin-8).
Since antihistamines often do not treat the
symptoms adequately, other mast cell mediators (prostaglandins, leukotrienes C4
and D4, bradykinin, and mast cell proteases) are apparently involved in
addition to histamine. A role of further immune cells and their mediators, for
example eosinophils, basophils or lymphocytes in urticaria, is also suspected.
Recent studies on pathogenesis are focusing
on the extrinsic coagulation system (formation of thrombin and fibrin) and the
enzyme matrix metalloprotease 9.
At least for chronic spontaneous urticaria,
a multifactorial model was developed in which the threshold for the development
of urticaria by increased mast cell activation is lower than in healthy
individuals. The lowering of the threshold until the development of urticaria
could be caused by intrinsic factors (genetic factors such as HLA association,
auto antibodies against FcεRI, or unknown factors). External factors such as
pseudo allergens or infections could increase the sensitivity of patients and
thus explain the variability of the clinical picture in individual patients.
Histology of urticaria
The histology of urticarial weals is usually non-specific and shows an
edema in the papillary and reticular dermis, dilatation of the small venules of
the upper dermis as well as a perivascular infiltrate with predominantly CD4-positive
T lymphocytes, monocytes and partially granulocytes (neutrophils, eosinophils,
basophils with individually different expressions) in a longer persisting hive.
The infiltrate is similar to a late-stage reaction. There is no epidermal
involvement. Dermal mast
cells in weals of chronic urticaria are increased by 10 times compared with non‐urticated
skin. Whether mast cell mediators such as
histamine or tryptase are elevated is also not clear. The cellular infiltrate
and cytokine pattern in patients with and without functional auto antibodies
against IgE or FcεRI are identical.
It is not possible to assess the severity, etiology, or
prognosis of urticaria in terms of course or response to therapy by
histopathology. Biopsies are therefore only useful to rule out differential
diagnoses such as urticaria vasculitis (typical: leukocytoclasia, erythrocyte
extravasates, deposits of fibrin, C3, IgG).
Clinical features of urticaria
The condition can present at any age. Acute urticaria is
common in young children with atopic dermatitis, but chronic urticaria peaks in
the fourth decade.
Itching
erythematous macules develop into weals and resolve within 2- 24 h, passing
through a macular erythematous phase, leaving the skin with a normal
appearance. The primary lesion
is the wheal, a palpably raised, sharply defined erythema and shows the
yellowish color of the serum exudate under pressure with a glass spatula. The
axon reflex (signals from skin receptors are also transmitted via collateral to
blood vessels) causes an erythema of varying width, around the individual
wheals: reflex erythema.
The size, number, and shape of each
weal can vary greatly. The typical weals develop within seconds to minutes and
usually disappear within 3–4 h. However, new weals may appear at a different
location. Usually hives are light red (Urtica rubra), but can also look
whitish anemic as a result of compression of superficial vessels by cutaneous
edema (Urtica porcellanea). They
may occur anywhere on the body, including the scalp, palms and soles and
variable in numbers and sizes, ranging from a few millimeters to lesions
covering large areas, and of varying shapes including rounded, annular,
flowerlike, serpiginous and bizarre patterns due to confluence of adjacent
lesions and they are usually heterogeneous. The heterogeneity of weals in size
and shape is one of the characteristics of spontaneous urticaria. Very rarely,
central blisters may form when edema is intense.
Itching (pruritus) is often described
as stinging or burning.
They may occur at any time, but often
appears in the evening or is present on waking. Irritation tends to be most intense at
night (parasympathetic
reaction)
and may disturb or prevent sleep. This, in turn, compounds the distress of the
condition. Patients tend to rub rather than scratch, so excoriation marks are
unusual, but occasionally bruising may result, which may be seen particularly
on thighs. Palmoplantar
tingling paresthesia, nausea, and dizziness indicate an incipient anaphylactic
reaction that may turn into anaphylactic shock. Women
may describe premenstrual exacerbations.
If the edema occurs in the subcutis, a circumscribed,
skin-colored swelling develops, angioedema, which are usually painful rather
than itching and can persist for up to 3 days when severe. Although angioedema
can also occur anywhere in the body, it is more common on the lids, lips, and
genitals, sometimes affecting the tongue, glottis, or larynx (early sign:
hoarseness) and can become life-threatening. The localization changes and is
usually asymmetrical.
Around
50% of patients with spontaneous urticaria describe angioedema associated with wealing at
some time of the illness and about 10% describe angioedema without weals.
Systemic symptoms of fatigue, lassitude,
sweats and chills, indigestion, myalgia or arthralgia may occur with severe
attacks, but the occurrence of pyrexia or arthritis should alert the clinician
to another explanation, such as urticarial vasculitis.
Classification
Urticaria is broadly classified by duration of disease and
clinical features. When urticaria is present daily or almost daily for less
than 6 weeks it is called acute. If urticaria occurs continuously on most days
lasting for 6 weeks or more, it is called chronic. The acute and chronic terminology is
usually applied to spontaneous urticaria but inducible urticarias may also be
acute or chronic, depending on their duration.
|
URTICARIA – CLINICAL
CLASSIFICATION AND DIFFERENTIAL DIAGNOSIS |
|
Clinical classification |
|
·
Spontaneous urticaria (all urticarias not
classified below) 1.
Acute 2.
Intermittent
(episodic) 3.
Chronic
(previously known as ‘idiopathic’) ·
Inducible urticarias 1.
Physical and cholinergic urticarias 2.
Contact urticaria (induced by percutaneous
or mucosal penetration)* |
|
Differential diagnosis |
|
·
Urticarial vasculitis (defined
histologically by leukocytoclastic vasculitis) ·
Angioedema without wheals (e.g. hereditary
angioedema, ACEi-induced angioedema) · Distinctive
urticarial syndromes (e.g. autoinflammatory syndromes) presenting with urticarial rash |
ACEi=
angiotensin-converting enzyme (
Classification
of the most common forms of urticaria
|
Spontaneous urticaria |
Inducible urticaria (physical forms) |
Inducible urticaria (special forms) |
|||
|
Subtype |
Definition |
Subtype |
Definition |
Subtype |
Definition |
|
Acute spontaneous
urticaria |
<6-week period of
spontaneous hives |
Symptomatic
dermographism (urticaria factitia) |
Occurs as a result
of mechanical shear forces (latency 1–10 min) |
Contact urticaria |
Occurs as a result
of contact with urticariogenic substance |
|
Chronic spontaneous
urticaria |
>6-week period of
spontaneous hives |
Cold urticaria |
Occurs as a result
of contact with cold (air/water/wind/objects) |
Cholinergic
urticaria |
Arises from
increased body temperature |
|
|
Heat urticaria |
Occurs as a result
of contact with local heat (air/water/wind/objects) |
Exercise-induced
urticaria |
Arises from physical
exertion |
|
|
Delayed pressure
urticaria |
Arises from vertical
pressure (latency 3–8 h) |
Aquagenic Urticaria |
Occurs as a result
of contact with water (temperature-independent) |
||
|
Solar Urticaria |
Arises from UV
and/or visible light |
|
|||
|
Vibratory
urticaria/angioedema |
Occurs through
vibration |
||||
The most common is the clinical
classification, which defines spontaneous urticaria and inducible urticaria
(physical urticaria and special forms). In contrast to spontaneous urticaria,
physical urticaria and special forms are also known as inducible
urticaria.
About 80% of urticaria is spontaneous, 10%
is physical, and less than 10% belong to a special form.
Two or rarely more urticaria types may
occur in the same patient (e.g., chronic spontaneous urticaria and symptomatic
dermographism or chronic spontaneous urticaria and delayed pressure urticaria).
In patients with two or more types of urticaria,
urticaria is usually protracted and difficult to treat.
Spontaneous urticaria
Acute versus Chronic
Urticaria
All urticarias are acute initially. Some will become chronic
after a period 6 weeks or more. The term “chronic urticaria” should only be
applied to continuous urticaria occurring at least twice a week off treatment.
Urticaria occurring less frequently than this over a long period is better
called episodic (or recurrent), because this presentation is more likely to
have an identifiable environmental trigger.
Acute
Spontaneous Urticaria
Definition
Acute spontaneous urticaria is defined as
spontaneous occurrence of hives, possibly accompanied by angioedema, over a
period of less than 6 weeks, 99% of cases persist only for a maximum of 3
weeks.
Epidemiology
Acute urticaria is the most common type of
urticaria and accounts for about one-third of all forms of urticaria and
two-thirds of spontaneous urticaria. Lifetime prevalence is between 15% and
20%. Younger age is more common, especially in children with atopic dermatitis.
Both sexes are affected approximately equally frequently. Due to the acute
appearance, acute urticaria is often seen in emergency rooms.
Etiopathogenesis
Most common is acute spontaneous
non-allergic urticaria, mostly in association with an acute
infection of the upper respiratory tract (30–62%), the urinary tract, and the
gastrointestinal tract, often in combination with a non-allergic
(pseudo allergic) reaction, e.g., the simultaneous use of nonsteroidal
anti-inflammatory drugs (especially cyclooxygenase I inhibitors such as
acetylsalicylic acid). The inhibition of the cyclooxygenase pathway by
nonsteroidal anti-inflammatory drugs leads to an increased accumulation of
leukotrienes instead of prostaglandins in the arachidonic acid metabolism, so
that the inhibitory influence of prostaglandin E2 on mast cell granulation and
leukotriene production is attenuated.
Acute spontaneous allergic urticaria may
also be caused by an IgE-mediated allergy (e.g., to food allergens). Although
most patients with acute spontaneous urticaria suspect an allergy to a food,
this is rarely the trigger and is more common in atopic patients, especially
small children with extrinsic atopic dermatitis (such as cow’s milk, hen’s
eggs, wheat, soy and peanut). Acute spontaneous allergic urticaria can also
occur in both atopic and non-atopic patients through medication (β-lactam
antibiotics) or hymenoptera stings (bee venom, wasp venom). Many patients has
an IgE-mediated type I allergy against a fish nematode Anisakis simplex been
reported as the trigger of acute urticaria (anisakiasis) after eating raw or
insufficiently cooked fish.
Clinical Features
The hives are mostly light red and larger
than 1 cm in diameter. In about 40% of patients, more than half of the body
surface is affected and systemic accompanying symptoms such as shortness of
breath (7%), exhaustion, nausea, or diarrhea occur.
Diagnostic Procedure
A specific diagnostic marker does not
exist. The diagnosis of acute urticaria is based on a careful history of
potential trigger factors (atopic diseases, known allergies, medication, food
intake, insect bites, and signs of infection) and a physical examination.
If no cause can be determined by history,
further examinations are not indicated in acute spontaneous urticaria due to
the self-limiting course of the disease.
Only the determination of a differential
blood count with erythrocyte sedimentation rate or C-reactive protein is
recommended as non-specific indicators of inflammation or infection. The
detection of a specific IgE-mediated sensitization (prick test, specific IgE
antibodies) should be performed if there are indications for an allergic
reaction.
Course
In more than 90% of cases acute spontaneous
urticaria shows a self-limiting course within 2–3 weeks without recurrence.
Although any chronic spontaneous urticaria must by definition have started as
acute urticaria, it is not possible to predict which patients will develop
chronic spontaneous urticaria. Adequate symptomatic therapy of acute
spontaneous urticaria may prevent progression to the chronic form.
Therapy
Trigger factors, such as allergens or drugs,
should be identified and avoided and infections adequately treated. Inpatient
admission is indicated in cases of shortness of breath, circulatory disorders,
and generalized, severe urticaria as well as threatening angioedema. The
primary symptomatic therapy for acute spontaneous urticaria consists of H1
antihistamines (in alphabetical order): bilastine, cetirizine, desloratadine,
ebastine, fexofenadine, levocetirizine, and loratadine. In the absence of a
response to the standard dose after 2 weeks an up to fourfold dose increase
should be considered (off-label use, potential side effects of the dose
increase should be considered). The second choice is the additional, short-term
administration of oral glucocorticoids (40–50 mg prednisolone equivalent per day
for 3–4 days).
In severe acute cases (associated severe
angioedema), initial intravenous administration of glucocorticoids (up to
100–250 mg prednisolone equivalent) in parallel with an antihistamine may be
required, even repeatedly. In the case of progression to anaphylactic shock,
the patient must be treated with epinephrine as soon as possible.
The administration of calcium has no
rational basis.
Acute
Spontaneous Urticaria in Childhood
Urticaria in childhood is usually acute spontaneous
urticaria. Angioedema is present in more than half of cases. The diagnostic
procedures as well as the therapy of acute spontaneous urticaria in childhood
do not differ fundamentally from the procedures in adults. In children,
especially infants with atopy, particular attention should be paid to potential
IgE-mediated triggers (especially food allergens such as cow’s milk, hen’s
eggs, soy, wheat, and fish). Cow’s-milk allergy is the commonest
cause of urticaria in infants under 6 months old. In infants, there may be less
itching and a greater tendency for weals to become purpuric. A common pattern
is one of bizarrely shaped weals, not seen as frequently in adults.
Newer H1 antihistamines, which are also
available as syrup, should be preferred to older preparations with more side
effects in children.
Causes of acute
urticaria

Potential allergic causes of acute
urticaria
·
Idiopathic
·
Infections
- Viral,
e.g. upper respiratory tract infections, hepatitis B and C
- Bacterial,
e.g. Streptococcus pyogenes
- Parasitic,
e.g. Anisakis simplex
·
Foods, e.g. cow's milk, hen's egg,
nuts, seeds
·
Drugs, e.g. β‐lactam antibiotics
·
Stings, e.g. bee, wasp venoms
·
Blood products, e.g. transfusions
·
Vaccines
·
Contactants, e.g. latex
Acute spontaneous urticaria
Allergic
Any drug, food,
foreign substance from blood transfusion, injection, implant, contactant and
inhalant should be considered as a potential allergen. Acute urticarial
reactions from drugs are common, usually occurring within hours of drug
administration in presensitized patients.
Acute
urticarial reactions to food are believed to be common and many go unreported.
Urticarial reactions may not be to the main food itself but to other
ingredients, such as seeds or spices. Rarely, allergic reactions to food occur
only if intake is followed by exercise, with neither food nor exercise alone
inducing weals (food‐dependent exercise‐induced
anaphylaxis). Substances reported to cause this include wheat, hazelnuts and
shellfish.
Non‐allergic
Histamine liberators
Mast cell
histamine release is non‐immunological and may occur after
first exposure. Examples include morphine, codeine, neuromuscular blocking
agents, such as atracurium, and antibiotics, such as polymyxin and vancomycin.
Iodinated radiocontrast dyes may cause non‐allergic anaphylaxis.
Pseudo allergic reactions
Common drug
causes include aspirin and other non‐steroidal anti‐inflammatory
agents. By inhibiting the cyclo‐oxygenase (COX‐1)
pathway of arachidonic acid metabolism, pro‐inflammatory lipoxygenase pathway
products leukotriene C4, D4 and E4 are
generated with inhibition of prostaglandin E2, which is inhibitory
for immunological mast cell degranulation.
Alcoholic beverages can aggravate
urticaria non‐specifically.
White wines are often treated with sulphites, which have rarely been reported to
cause urticaria and anaphylaxis. Some red wines contain measurable
concentrations of vasoactive amines including histamine, which could aggravate
urticaria.
Food may also contain vasoactive
amines including histamine (such as in cheese, fish, processed meat, tomatoes,
pineapple and avocados) or histamine‐releasing substances (such as in strawberries). Histamine
generated in scombroid fish (under processed tuna) by histidine decarboxylase
from bacteria can cause acute flushing, urticaria, vomiting and diarrhea. High
levels of histamine can usually be found in affected fish.
Infections
Urticaria may follow non‐specific viral infections, or acute
hepatitis B viral infections, anisakiasis (infection by a fish parasite in
presensitized individuals), streptococcal throat infections in children.
CHRONIC SPONTANEOUS URTICARIA
Definition
If spontaneous hives persist daily or almost daily over a
period of more than 6 weeks, then chronic spontaneous urticaria is present. If
the course is characterized by intermittent and not daily symptoms the
urticaria is called episodic urticaria (intermittent urticaria);
an IgE-mediated cause should then be excluded.
Epidemiology
The lifetime prevalence of chronic spontaneous urticaria
is 1–2%. Usually middle-aged people (20–60 years) are affected, with females
twice as frequently. In contrast to acute spontaneous urticaria, atopy is not a
predisposing factor.
Etiopathogenesis
The causes of mast cell activation in chronic spontaneous
urticaria are complex and multifactorial. IgE-mediated sensitization is
extremely rarely the cause of symptoms. However, many direct and indirect
factors that activate mast cells may be involved, such as autoreactive
mechanisms (autoantibodies against FcεRI or IgE or unknown epitopes),
infectious diseases (viral, bacterial, parasitic) – in particular Helicobacter
pylori-associated gastritis, pseudo allergic reactions (to nonsteroidal
anti-inflammatory drugs or food additives) and other such as psychoneurological
factors or very rarely hematologic or lymphoproliferative diseases or others
malignancies. It is not uncommon to find several factors in one patient.
Approximately one-third of patients with chronic
spontaneous urticaria show evidence for auto reactive mechanisms through
functionally mast cell-stimulating IgG antibodies against the α chain of the
high affinity IgE receptor (FcεRI), rarely also against IgE itself. If the
autologous serum skin test is positive, autoimmune thyroiditis with thyroid
auto antibodies is more common (about 30% of patients with chronic spontaneous
urticaria).
Pseudo allergens (substances that cause IgE-independent,
dose-dependent mast-cell activation with an unclear mechanism without a preceding
sensitization phase) like acetylsalicylic acid, other nonsteroidal
anti-inflammatory drugs and as mast-cell activating drugs (histamine
liberators) such as morphine, codeine, muscle relaxants, radiocontrast media,
and dextran can aggravate the symptoms of urticaria and trigger exacerbations.
Non-allergic hypersensitivity reactions to individual food additives such as
(azo) dyes, preservatives, or antioxidants are rather rare.
A causal role of chronically persistent infections has
not yet been clearly proven, but long-standing urticaria complaints often
disappear after eradication of a focus (Helicobacter pylori-gastritis;
streptococci or staphylococci: chronic tonsillitis, sinusitis, dental
infections; persistent Yersinia enterocolitica infection; infestation
with Blastocystis hominis, Giardia lamblia, Entamoeba histolytica).
Best documented is the association of chronic spontaneous urticaria with Helicobacter
pylori-associated gastritis. After eradication, about twice as many
patients show complete or significant improvement of their urticaria compared
to non-eradicated Helicobacter patients. In principle, patients with chronic
spontaneous urticaria do not have infections more frequently than controls, but
seem to be particularly susceptible to the development of urticaria. Potential
pathomechanisms include bacteria-specific IgE, molecular mimicry of bacterial
antigens with the induction of auto antibodies and permeability changes due to
the inflammatory reaction.
About half of those affected also report that psychoneurological
factors such as stress, especially acute stress situations, worsen the
symptoms. So far, it is unclear whether the psychopathological abnormalities
are primarily present or are caused reactively, for example, through a central
nervous effect of histamine.
Clinical Features
The hives in
chronic spontaneous urticaria are usually bright red and round with a variable
diameter of one to several centimeters. In more than 50% of patients,
angioedema occurs in addition to the hives, in about 30% only hives, and in 10%
angioedema without hives.
Urticaria and/or angioedema can occur anytime and anywhere
on the skin, most often in the evening and on the extremities. Angioedema can
also occur spontaneously at night and is usually located on the head
(especially the eyelids, lips, tongue), but also on the hands, feet, and
genitals. Accompanying symptoms such as fever, headache, arthralgia, or
gastrointestinal symptoms, but also shortness of breath, are possible. In 10%
of patients, symptoms occur daily. Quality of life is significantly impaired
due to severe itching, sleep disorders, and secondary psychosocial problems.
Differential Diagnosis
In itchy, urticarial skin lesions, differential
diagnostic urticarial stages of bullous autoimmune skin diseases (especially
bullous pemphigoid), scabies and other arthropod reactions, early stages of
vasculitis and erythema multiforme, in pregnancy also polymorphic eruption of
pregnancy or pemphigoid gestationis, must be considered.
The conceptually confusing clinical picture of urticarial
dermatitis, which mostly occurs in older patients and is accompanied by plaques
persisting for longer than 24 h, severe itching with partly urticarial, partly
eczematous morphology, is a diagnosis by exclusion. The distribution is mostly
bilateral and symmetrical on the trunk or the proximal extremities. Histology
shows a predominantly dermal eczematous reaction with edema in the papillary
layer, superficial perivascular infiltrate with eosinophils and minimal epidermal
spongiosis. The cause can be a drug reaction or an undefined dermatitis. The
epidermal involvement allows differentiation from urticaria.
In case of non-itchy hives and lack of response to H1
antihistamines, autoinflammatory syndromes with urticaria-like
skin changes have to be considered for differential diagnosis. Autoinflammatory
syndromes differ from autoimmune diseases in the absence of autoantibodies or
autoreactive lymphocytes. Autoinflammatory syndromes are characterized by
persistent or recurrent fever.
Schnitzler syndrome with arthralgia, fever attacks,
monoclonal IgM-gammopathy is a non-hereditary autoinflammatory syndrome.
Antagonistic antibodies against cytokines are available for some
autoinflammatory syndromes (IL-1 receptor antagonist Anakinra has been
successfully described in Schnitzler syndrome, IL-1β antibody Canakinumab is
approved for CAPS).
Diagnostic Procedure
The diagnosis is based on a careful and structured
history considering potential trigger factors. A complaint diary to be kept by
the affected person with additional documentation of food, medication, and
activities is helpful. Diagnostics encompass physical examination including
dermographism, laboratory examinations, and, if necessary, additional further
assessments such as consultative examinations (dental, ENT, gynecological) or
imaging procedures (x-ray/computer tomography of paranasal sinuses,
sonography).
Routine prick tests for inhalation and food allergens are
of low diagnostic value. A biopsy is recommended if differential diagnoses are
suspected (especially urticaria vasculitis, bullous pemphigoid). If physical
urticaria is suspected, standardized physical tests must be carried out.
Any attempt to find a cause or trigger factor is
advisable because identification and elimination is the best therapeutic
strategy. This applies in particular to chronic spontaneous urticaria that has
existed for more than 6 months.
It is
recommended that the severity of the disease be determined on the basis of an
established daily urticaria activity score (UAS), which is often determined for
7 days (UAS7).
Urticaria
activity score (UAS)
|
Findings |
Points |
|
How many wheals have occurred in
the last 24 h? |
|
|
None |
0 |
|
Few (<20) |
1 |
|
Many (21–50 hives) |
2 |
|
Very many (≥50 hives or large
confluent areas) |
3 |
|
How strong has the itching been in
the last 24 h? |
|
|
No itching |
0 |
|
Mild (present but not annoying or
troublesome) |
1 |
|
Moderate (troublesome but does not
interfere with normal daily activity or sleep) |
2 |
|
Intense (severe pruritus, which is
sufficiently troublesome to interfere with normal daily activity or sleep) |
3 |
|
Urticaria activity score (UAS) of
1 day |
Sum of points (0–6) |
|
UAS7 = Total score for a week
(maximum 42 points) |
|
Another new
system, which has been established and validated in recent years, has proven to
be particularly practical: Urticaria Control Test (UCT).
This is suitable for assessing disease activity of the last 4 weeks of all
patients with chronic urticaria (CSU and CINDU) and for monitoring therapy
decisions through standardized and reliable documentation. The UCT consists of
four questions, each with five possible answers. The higher the score, the
better under control the urticaria is. Good control can be assumed from a
cut-off value of 12 points. If the value is less than 12, treatment should be
optimized.
Urticaria
Control Test (UCT)
|
Question |
Reply |
Points |
|
1. How much have you suffered from
the physical symptoms of the urticaria (itch, hives and/or swelling) in the
last 4 weeks? |
Very much Much Somewhat A
little Not at all |
0 1 2 3 4 |
|
2. How much was your quality of
life affected by the urticaria in the last 4 weeks? |
Very much Much Somewhat A
little Not at all |
0 1 2 3 4 |
|
3. How often was the treatment for
your urticaria in the last 4 weeks not enough to control your urticaria symptoms? |
Very often Often Sometimes Seldom Not at all |
0 1 2 3 4 |
|
4. Overall, how well have you had
your urticaria under control in the last 4 weeks? |
Not at all A
little Somewhat Well Very well |
0 1 2 3 4 |
Cut-off value 12 points or higher: Good
control can be assumed
Cut-off values <12: urticaria is not
controlled, treatment should be adapted
Routinely laboratory determination of only a differential
blood count as well as of erythrocyte sedimentation rate or C-reactive protein
as a coarse grid on inflammatory/infectious processes is recommended. Further
diagnosis depends on patient history as well as the clinical picture.
Proven
diagnostics procedures for chronic spontaneous urticaria
|
Examination
for |
In
detail |
Method |
Remark |
|
Infection |
General information |
Differential blood count C-reactive protein or erythrocyte sedimentation rate |
|
|
Helicobacter pylori |
Monoclonal stool antigen test
or C-urea breath test or histopathology |
The non-invasive monoclonal stool
antigen test is very sensitive; observe waiting periods for taking antacids
and proton pump inhibitors as well as antibiotics Serology is not reliable |
|
|
Streptococci |
Anti-DNaseB titer,
Anti-Streptolysin titer (throat swab) |
|
|
|
Staphylococci |
Anti-Staphylolysin Titer |
|
|
|
Yersinia enterocolitica |
Yersinia serology (IgA, IgG,
immunoblot) |
IgA and several bands in
immunoblot indicate persistent yersiniosis |
|
|
Autoreactive |
Autoimmune thyroiditis |
Basal TSH Thyroperoxidase
antibodies Thyroglobulin
antibodies TSH-receptor autoantibodies |
If basal TSH is abnormal, FT3 and
FT4 should be assessed. |
|
FcεRI (IgE), serum factor(s) |
Autologous serum test |
Direct Anti-FcεRI autoantibody
assay are not commercially available. Serum functional tests such as
histamine release, leukotriene production, CD63 or CD203c expression are too
complex in routine. |
|
|
Pseudoallergy |
Nonsteroidal anti-inflammatory
drugs |
Anamnesis, avoidance |
Alternatives: paracetamol, tramadol, etoricoxib; oral provocation test at urticaria free intervals, if
necessary |
|
Food additives |
Standardized low pseudo allergen
diet for 4 weeks |
If applicable, blinded oral
provocation test with pseudo allergen-rich food, collective additives,
exposure |
Other possible
diagnostic measures that are not routinely required are:
·
Antinuclear
antibodies (preferably in urticaria vasculitis to exclude lupus erythematosus)
·
Stool on worm
eggs (eosinophilia, increased total IgE, suspected parasitosis)
·
Biopsy (e.g.,
of lesions that persist in loco for more than 24 h, for differential diagnosis
of urticaria vasculitis, urticarial dermatitis, bullous pemphigoid, cutaneous
mastocytosis)
·
Basal serum
tryptase (to differentiate mastocytosis)
·
Specific IgE
antibodies (if IgE-mediated mechanisms are suspected)
The most common
test for determining autoreactivity is the autologous serum test since
commercially available tests for the determination of auto antibodies against
IgE or FcεRI are not available and functional tests (histamine release test,
sulfide-leukotriene production or flow cytometric determination of activation
markers such as CD63 on basophils) are reserved for specialized centers within
the scope of studies due to the logistical effort involved. The result is
currently only used to subclassify chronic spontaneous urticaria into
autoreactive and non-autoreactive. A therapeutic consequence has not yet been
established.
In the case of inconspicuous basic diagnostics, an outpatient 4-week
standardized low-pseudo allergen diet may be tried under qualified nutritional
consultation. If there is a significant improvement in symptoms, an inpatient
provocation test with standardized pseudo allergen-rich food, collective
exposure to food additives, and individual substance breakdown should be
considered. Overall, about one-third of the patients benefit from the diet, but
complete freedom from symptoms is rarely achieved and a subsequent provocation
test is rarely conspicuous. After 3–6 months of a strict pseudo allergen-low
diet, most patients will be able to tolerate the gradual intake of food again.
Course
Chronic spontaneous urticaria persists on average for 3–5 years; only
half of those affected show remission within 10 years.
Therapy
The aim of the therapy is complete freedom from symptoms.
Strategies include elimination or avoidance of the trigger (e.g., eradication
of Helicobacter pylori), inhibition of mediator release from mast
cells (glucocorticoids, phototherapy, cyclosporin A), and inhibition of
mediator action at the target organ (H1 antihistamines, leukotriene receptor
antagonists).
General Recommendations for Urticaria
·
Elimination of
causal factors
·
Avoidance of
nonsteroidal anti-inflammatory drugs (acetylsalicylic acid) or mast
cell-activating drugs
·
Avoidance of
ACE inhibitors, AT-II receptor antagonists (only in recurrent angioedema)
·
Avoiding
overheating, alcohol, stress
·
Topical antipruritic
treatment (polidocanol 3–5%), cooling lotions
·
In case of
threatening angioedema, anaphylaxis: carry emergency medication with you.
In addition to avoiding nonspecific activating factors,
identified persistent bacterial (Helicobacter pylori infection) or
parasitic infections should be treated, as this can lead to complete freedom
from symptoms. The success of the therapy should be investigated (antibiotic
resistance of Helicobacter pylori is known). Urticaria often
only responds after a delay of 8–12 weeks of eradication therapy. For thyroid
auto antibodies, therapy may be indicated for thyroid dysfunction, but has no
effect on urticaria. In case of improvement under a low pseudo allergen diet a
gradual relaxing of the diet after 3–6 months can be tried. A specific therapy
in case of a positive autologous serum test and/or the presence of auto antibodies
against FcεRI is not yet available.
Topical treatment is not very effective, but is often
used by some patients in addition to systemic therapy. Suitable products are
itch-relieving and cooling substances, for example polidocanol-containing
(3–5%) lotions or creams. Topical antihistamines are not recommended due to
their sensitizing potential.
Symptomatic standard therapy for the first stage
consists of non-sedating or less-sedating histamines due to the central
importance of histamine. H1 antihistamines (in alphabetical
order) are: bilastine, cetirizine, desloratadine, ebastine, fexofenadine,
levocetirizine and loratadine, in standard dosage. There have not been many
direct comparative studies of chronic urticaria between these H1
antihistamines. In the two studies in which a comparison of desloratadine with
levocetirizine was investigated, levocetirizine performed better.
They block the histamine effect at the H1 receptor and
thus stop itching, erythema, and wheals. Taken regularly and, if necessary,
spread over the day is more effective than taken as needed. Older H1
antihistamines (e.g., hydroxyzine) should only be used if sedation is expressly
desired, especially due to the usually required dose increase. Their negative
influence on the REM sleep phase, learning, and mental performance must be
taken into account.
Recommended
four-stage symptomatic treatment algorithm
according to evidence and consensus
·
Stage one:
·
Standard dose
of second-generation H1 antihistamine
·
If inadequate
control: after 2–4 weeks or earlier, → stage 2
·
If symptoms are
intolerable → stage 2
·
Stage two:
·
Dosage increase
of the second-generation H1 antihistamine up to fourfold (off-label)
·
If inadequate
control: After 2–4 weeks or earlier, if symptoms are intolerable → stage 3
·
Stage 3 (in addition to stage 2):
·
Add omalizumab
·
If inadequate
control: Within 6 months or earlier, if symptoms are intolerable → stage 4
·
Stage 4 (in addition to stage 2):
·
Add cyclosporin
A
·
In
exacerbations systemic glucocorticoids are possible for a short time (maximum
10 days).
·
Stages 3 and 4
should be performed under the supervision of a specialist
With the standard dose of H1 antihistamines and also with
a dose increase of up to four times (off-label) complete freedom from symptoms
can only be achieved for a small number of patients.
If there is no response to the standard dosage within 2
weeks, the second stage with an up to fourfold increase in dosage
(off-label use) taking into account potential side effects is recommended. Due
to the individual responses, a change to another H1 antihistamine should also
be considered.
In case of further therapy resistance within the next 2–4
weeks, treatment is progressed to the third stage as add-on therapy
to the second stage using omalizumab.
If within 6 months or earlier, if symptoms are
intolerable, and omalizumab add-on is not effective, stage four cyclosporin
A (off-label, dose 2.5–5 mg/kg body weight per day, response within 4–6 weeks)
should be added to second generation H1 antihistamines (stage 2)
The risk-benefit profile should be carefully weighed
against other off-label alternatives (dapsone, montelukast, H2 antihistamines)
due to the low level of evidence.
Omalizumab has been approved for the indication of chronic
spontaneous urticaria that does not respond to antihistamines. About half of
patients with chronic spontaneous urticaria respond after only two injections
(mean time to response 6 weeks). However, some patients (about 15%) need more
than 6 months until urticaria symptoms are controlled. Casuistically, in case
series and for some subtypes such as cholinergic urticaria, double-blind
controlled trials have demonstrated efficacy with omalizumab in chronic
inducible urticaria. After weaning from omalizumab, however, a relapse usually
occurs just as quickly, so it is a symptomatic therapy. The mechanism of action
of omalizumab (anti-IgE antibody) is still unknown. The rapid success speaks
against a down-regulation of high-affinity IgE receptors on mast cells. The
hypothesis that anti-IgE treatment captures IgE autoantibodies have not been
proven so far. Recently, a randomized phase II clinical trial has demonstrated
safety and efficacy of ligelizumab, an anti-IgE antibody with increased
affinity to the IgE-receptor, compared to placebo and omalizumab in chronic
spontaneous urticaria.
For cyclosporin A evidence for efficacy
and safety in the indication H1 antihistamine-resistant chronic urticaria is available
from randomized controlled trials. H2 antihistamines were
investigated only in combination with sedating H1 antihistamines in studies
with contradictory results. Dapsone may be more suitable for
pronounced inflammatory infiltrates with neutrophils and/or eosinophils
(pressure-associated chronic spontaneous urticaria or delayed-pressure
urticaria). Other therapies successful in smaller studies or individual cases
are (hydroxy)chloroquine, sulfasalazine, tacrolimus, methotrexate,
mycophenolate mofetil, cyclophosphamide, and photo treatment with UVB 311 nm.
Systemic glucocorticoids should be used for a maximum of
10 days for acute exacerbations; the initial recommended daily dose is 0.5–1
mg/kg body weight prednisolone equivalent. There should be regular checks every
3–6 months to see whether it is possible to reduce the dose or discontinue
medication if spontaneous remission has occurred.
Chronic
Spontaneous Urticaria in Childhood
Chronic spontaneous urticaria in childhood is less common
than in adults. The diagnostic procedure as well as the therapy of chronic
spontaneous urticaria in childhood does not differ from those in adults.
Trigger factors are comparable, with persistent streptococcal infections being
most common. As with adults, one-third has a positive autologous serum test. A
weight-adapted dose increase of modern H1 antihistamines is also recommended
for children who do not respond to the standard dose. Omalizumab is approved
for the indication of chronic spontaneous urticaria from the age of 12 years.
Alternatives such as montelukast and cyclosporin A are generally approved in
childhood.
Causes of chronic
urticaria:
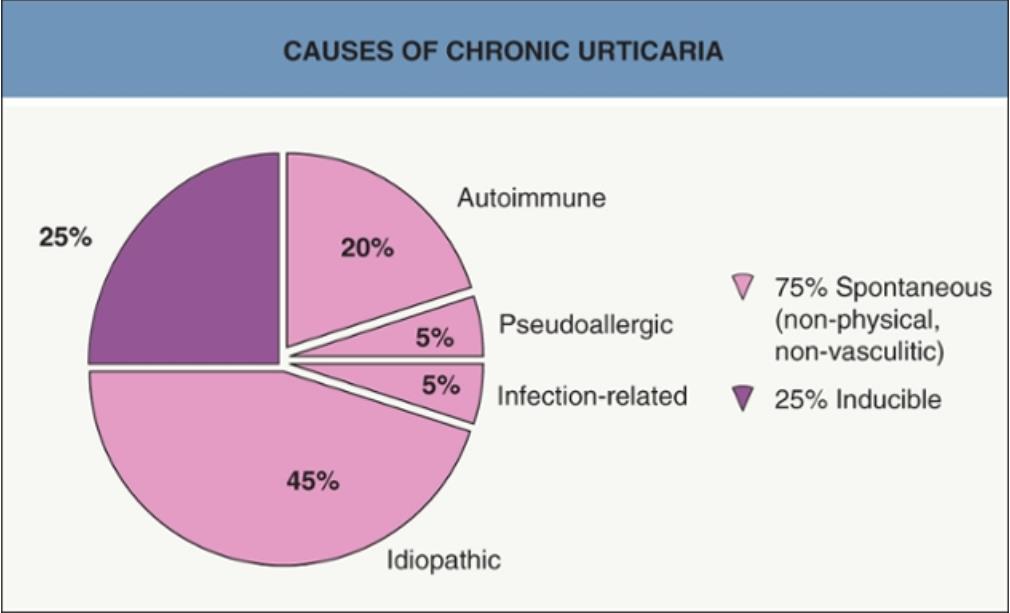
Autoimmune
represents those patients with functional autoantibodies against FcϵRI or the
Fc portion of IgE.
Chronic spontaneous urticaria
Idiopathic
At least 50% of
patients with chronic spontaneous urticaria are idiopathic.
Allergy
IgE‐mediated
allergy is probably never the cause of chronic spontaneous urticarial.
Autoimmune
Patients with autoimmune
urticarial who have functional autoantibodies are more likely to respond
to immunosuppressive therapies.

The
pathogenesis of autoimmune urticarial and the proposed mechanism of action of
omalizumab for autoimmune urticaria.
Pseudo allergy
Food additives, natural salicylates,
amines, spices, green teas and alcohol may aggravate existing chronic
spontaneous urticaria in up to 30% of patients but are rarely the cause. A 3‐week trial of a low pseudo allergen
diet may be considered as a diagnostic investigation in well‐motivated patients.
Infections
and infestations
Bacterial infections, such as dental
sepsis, sinusitis, urinary tract and gallbladder infections, may be associated
with chronic urticaria. If present, treatment of the infection usually does not
cure urticaria. Helicobacter pylori infection of the stomach has been
associated with chronic spontaneous urticaria.
Duration of Hives
|
Type of Urticaria |
Duration |
|
Spontaneous and delayed pressure |
4-36 hours |
|
Physical (except delayed pressure) |
30 min-2 hours |
|
Contact (may have a delayed phase) |
1-2 hours |
|
Urticarial vasculitis |
1-7 days |
Aggravating
factors
Even though a specific cause of
urticaria may not be identified in individual patients, it is often possible to
identify non‐specific
aggravating factors in chronic urticaria, such as heat and clothing pressure in
spontaneous urticaria, avoidance of which can help to minimize exacerbations.
Aggravating factors
for spontaneous urticaria
·
Physical
o Pressure
o Overheating (passive or active)
·
Infections, e.g. upper respiratory
tract infections
·
Drugs
o Non‐steroidal
anti‐inflammatory
drugs (common)
o Opiates (rarely)
·
Dietary pseudo allergens
o Natural salicylates
o Histamine
o Food additives
o Spices
o Alcohol
·
Menses (premenstrual especially)
·
Stress
Pressure
and heat
Patients often volunteer that weals come up below tight clothing
or after overheating.
Drugs
Aspirin and other related non‐steroidal anti‐inflammatory drugs (NSAIDs), such as diclofenac, can
aggravate urticaria by non‐allergic
mechanisms.
Dietary pseudo allergens
The most frequently implicated food additives are tartrazine
(E102) and other azo dyes, including sunset yellow (E110).
Infections
Chronic urticaria is frequently exacerbated by intercurrent
viral infections. This may be a non‐specific effect of circulating pro‐inflammatory cytokines or
chemokines.
Menstrual
cycle and pregnancy
Urticaria may worsen premenstrually, but if urticaria occurs
predominantly or only premenstrually, it has been attributed to progesterone
sensitivity.
Stress
Flare‐ups
of urticaria do occur at times of psychological stress.
Inducible Urticarias
The inducible urticarias represent a distinct subgroup of the
urticarias that are induced by an exogenous physical stimulus rather than
occurring spontaneously. These include
physical forms of urticaria triggered by external mechanical stimulation, such
as pressure, cold, heat, and special forms (contact urticaria, cholinergic
urticaria and aquagenic urticaria). Exercise-induced urticaria/anaphylaxis is
mostly associated with an IgE-mediated allergy to food (mostly wheat, rarely
shellfish or others), and is therefore classified as food allergy or
anaphylaxis and no longer as chronically inducible urticaria.
The physical urticarias are classified by the predominant
stimulus that triggers whealing, angioedema or anaphylaxis. Of all the
urticarias, delayed pressure urticaria and cholinergic urticaria may affect the
quality of life most severely. While the lesions of most physical urticarias
occur within minutes of provocation and generally resolve within 2 hours, a few
physical urticarias (e.g. delayed pressure urticaria, delayed dermographism)
develop after a delay of several hours and persist for 24 hours or longer.
The weals are usually localized to the stimulated area of
skin. However, sometimes the physical stimuli need to produce a systemic
effect, e.g. a rise or drop in core body temperature, to induce urticaria of a
reflex type. Thus, generalized heating of the body can induce cholinergic
urticaria (which is common), and generalized cooling, cold reflex urticaria (which
is rare). Here, multiple small wheals occur on
widespread areas of the body.
Angioedema
may be seen with all the physical urticarias except with symptomatic
dermographism. Vibratory angioedema manifests with subcutaneous swellings but
not wheals. Also, several forms of physical urticaria can coexist in the same
patient. Common combinations include: (1) symptomatic dermographism and
cholinergic urticaria; (2) cold and cholinergic urticaria; and (3) delayed
pressure urticaria and delayed dermographism. Delayed pressure urticaria may
also coexist with chronic urticaria.
Most chronic inducible
urticaria forms persist for 3–5 years or longer.
Diagnosis is made through
careful history, clinical examination, and standardized physical testing.
Dermographism
After light, linear striation of the skin
with a hard object (wooden spatula, pin), the touched area reddens in a line
within 15–20 s due to reflective vasodilation: red dermographism (Dermographismus
ruber). In patients with atopic diathesis or atopic diseases, however,
vasoconstriction often results in white dermographism (Dermographism
albus). In atopic eczema, white dermographism is one of the minor
diagnostic criteria.
This
is divided into simple or symptomatic.
An urticarial reaction occurs within 5 min
in the contact area and slightly beyond without itching, which can last for
minutes to more than 1 h. in response to moderate stroking of the skin and
may be regarded as an exaggerated physiologic response. This asymptomatic Simple immediate urticarial dermographism has no disease
value and occurs in about 5% of the population. The very rare urticarial
late dermographism develops only after 3–6 h and can last
up to 24 h.
Symptomatic immediate dermographism is the
most common type of physical urticaria. It manifests as linear wheals at sites
of scratching or sites of friction, such as collars and cuffs of clothes.
Whealing occurs after gentle stroking of the skin in response to a shearing
force. Patients, most frequently young adults, often complain of pruritus
before the wheals appear and may not associate them with scratching. The
itching is often disproportionately severe compared with wealing, is worst in
the evening and often occurs in bouts. The lesions usually resolve within an
hour. Mucosal involvement does not occur, but vulvar swelling during sexual
intercourse has been reported. As a rule, the hives are not round, but arranged in a line or stripe
according to the stimulus (writing on the skin is possible). Since wheals
caused by rubbing can cause itching again, a vicious cycle is triggered. The general course is
unpredictable, but usually there is a gradual tendency towards improvement over
several years. Symptomatic dermographism is usually idiopathic, but occasionally
follows scabies infestation and penicillin allergy. There is no association
with systemic disease, atopy, food allergy, or autoimmunity. Similar to an urticarial late
dermographism, a delayed and long-lasting symptomatic dermographism can also
occur.
Symptomatic dermographism lasts an average of 6.5 years.
Chronic spontaneous urticaria or another inducible urticaria is often found in
combination.
Symptomatic dermographism is most easily diagnosed by
using a calibrated instrument, the dermographometer, which has a spring-loaded
stylus, the pressure of which can be adjusted to a predetermined setting.
Stroking the skin at a tip pressure of less than 36 g/mm2 induces a linear,
itching weal within 10 min.
Treatment of symptomatic immediate dermographism with
low-sedating H1 antihistamines is often effective, sometimes in low doses.
Delayed pressure urticaria
Delayed
pressure urticaria (DPU) is important because it can interfere severely with
quality of life and its treatment is difficult. Delayed pressure
urticaria is uncommon (2% of urticarias). Up
to 37% of patients with chronic spontaneous urticaria have associated DPU.
Conversely, nearly all patients with DPU have associated spontaneous wheals.
Because of this association and the delayed onset, patients may not be aware of
any relationship to pressure unless specifically questioned.
Wealing occurs at sites of sustained vertical pressure
applied to the skin after a delay of 30 min to 9 h, but usually 4–8 h, and
lasts 12–72 h; sometimes it resembles angioedema. These
deep swellings may be itchy, but are often tender or painful.
Sites frequently involved are the waistline after wearing
tight clothing, below the elastic of socks, on the buttocks and lower back after sitting,
the feet in tight shoes, the palms
after manual work, the soles after walking or climbing ladders, and the genitalia
after intercourse.
DPU may be accompanied by systemic symptoms of malaise,
flu-like symptoms, arthralgia and myalgia. The condition may be mistaken for
urticarial vasculitis.
The diagnosis can usually be made by careful questioning
and confirmed by testing. Objective testing is performed by using rods with a
convex end diameter of 1.5 cm weighted with 2.5 kg for 20 min or 4.5 kg for 15
min on the back or thighs. A positive response is when indurated lesions are
present at test sites at 6 h. Areas of delayed pressure urticaria may be
refractory to further pressure-induced lesions for up to 48 h.
The average duration of delayed pressure urticaria is 6–9
years.
The differential diagnosis is a pressure-aggravated
chronic spontaneous urticaria in which whealing occurs not only spontaneously
but is also pressure-associated (mostly in pressure-loaded areas, or the belt
area). The wheals often only appear after 30 min in the pressure test, but are
not delayed for several hours.
Histopathology
In delayed-pressure urticaria, a biopsy from a
pressure-induced wheal may be useful. The infiltrate is more pronounced than in
other forms of urticaria; histopathologically a differentiation from urticaria
vasculitis is possible. Early lesions (<5 h) are dominated by neutrophils
and eosinophils, late lesions (>12 h) are more likely to have lymphocytes
and eosinophils. The underlying swellings are also considered
histamine-mediated, whereby the expression of adhesion molecules on endothelial
cells and the neutrophil- and eosinophil-rich infiltrate indicate a role of
cytokines.
As far as possible, vertical pressure should be avoided
(by padding the affected area).
Delayed pressure urticaria responds poorly to
H1 antihistamines but higher than licensed doses of cetirizine (10 mg three
times a day) have been used, as it also inhibits eosinophil migration. Some patients benefit from additional
administration of medium to low doses of glucocorticoids (40–20 mg prednisolone
equivalent or less). Drugs
that inhibit granulocyte infiltration (including colchicine, dapsone and
sulphasalazine) may be helpful although supporting clinical studies are
lacking. Dapsone (50–150
mg daily, 6 days per week) has been described in case series as being
successful. Further options are methotrexate (15 mg/week), montelukast (10
mg/day), sulfasalazine (up to 3 g/day). The use of topical clobetasol propionate 0.5% under occlusion for
the hands and feet may be effective and wearing comfortable shoes or insoles
can be useful. Omalizumab has
also been described as successful in individual cases.
Cholinergic
urticaria (sweating induced)
It accounts for about
5% of urticaria. Small weals begin within
15 minutes after
the patient experiences a general overheating of the body as a result of sweat-inducing stimuli, whether induced by a rise in core
temperature, emotion or gustatory stimuli, such
as any form of physical exertion, hot baths or sudden emotional stress, moving
from a cold to a hot room, drinking alcohol and eating spicy food. It occurs
more frequently in adolescents
and young adults with an atopic diathesis and may be worse in the winter months and is unusual in the elderly.
After the appropriate stimulus, pruritus is
followed by the development of multiple, small, 2- to 3-mm dome-shaped monomorphic
wheals
with a pale center and surrounded by obvious erythematous flare that are symmetrically distributed. They are most prominent
on the upper half of the body such as
face and trunk but can also affect the lower legs and
forearms and even become generalized. Oblique lighting is
helpful for observing the weals, especially in dark skin. The lesions persist
for a few minutes to an hour or two. Angioedema and
systemic manifestations consisting of faintness, headache, palpitations,
abdominal pain, and wheezing may occur.
Cold urticaria, symptomatic dermographism, or
aquagenic urticaria may be associated with cholinergic urticaria. There is
usually a gradual tendency towards improvement, but the condition may last for
years. Rarer forms include cholinergic pruritus, cholinergic erythema (in which
pruritic, symmetric, small erythematous macules appear to be persistent, but
individual lesions actually last for up to 1 hour), and cholinergic
dermographism. Severe exercise-induced cholinergic urticaria may sometimes
progress to anaphylaxis.
The most reliable and efficient testing method is to ask
the patient to run in place or to use an exercise bicycle for 15 minutes, and
then to observe the patient for 1 hour to detect the typical micropapular
hives. Exercise testing should be done in a controlled environment. Patient is
asked to take a hot bath at 40-42°C for 15 min to raise the core temperature by
0.7 to 1°C—and induce characteristic micropapular hives. A few patients find
that if they can bring on a severe attack by suitable exertion they can achieve
freedom for up to 24 h afterwards, analogous to temporary desensitization.
If wheals only occur with bathing, an aquagenic urticaria
or a heat urticaria should be considered. If, on the other hand, only the
exercise test is positive, exercise-induced urticaria (e.g., wheat-dependent
exercise-induced urticaria/anaphylaxis) must be ruled out.
Therapeutically, modern H1 antihistamines (possibly
off-label in increased dosage) are used prophylactically regularly or 30–60 min
before typical situations. Not infrequently, symptoms are only partially
suppressed by this. Tolerance induction for physical exertion is difficult to
achieve. Omalizumab has been shown to be effective in a randomized double-blind
controlled trial. Optional drugs with low evidence levels include ketotifen,
danazol, H2 antihistamines, montelukast, doxepin, β-blockers, or prednisolone.
The average duration of cholinergic urticaria is 7.5
years. Progressions over 30 years have been described.
Primary cold contact urticaria
This is by
far the commonest form, occurring at any age but most frequently in young
adults. Although It may be preceded by non‐specific
upper respiratory tract viral infections, arthropod
bites or stings, the cause of most cases remains unknown (idiopathic).
Itching and wealing occur in cold-exposed areas after contact with cold objects,
cold water or cold air within minutes of
rewarming the skin after cold exposure and last up to 1 h. Cold winds
and cold rain are particularly effective stimuli. Sometimes, the mouth and
pharynx may swell after drinking cold liquids. Systemic
symptoms of flushing, headache, syncope, and abdominal pain can develop if
large areas are affected. Cold baths and swimming should usually be avoided as
there is a potential risk of anaphylaxis.
The
mean duration of cold urticaria is 5–10 years, though primary cold contact
urticaria may be more transient if it follows a viral infection.
Diagnosis is made by application of a melting ice cube in a
thin plastic bag onto the skin for 5–20 min, and wealing occurs within 10 min,
usually during rewarming.
A distinction is made between primary, acquired cold
urticaria (an allergic type I reaction) and secondary cold urticaria with
detection of cold-sensitive serum proteins (cryoglobulins, cold agglutinins,
cryofibrinogen) in about 2% of those affected, possibly in the context of
malignant lymphoma or leukaemia or in the case of infectious disease
(borreliosis, HIV infection/AIDS, infectious mononucleosis).
To exclude secondary cold urticaria in infectious
triggers such as borreliosis, infectious mononucleosis, and HIV infection,
serological tests should be performed, as well as tests for cryoglobulins, cold
agglutinins, and cryofibrinogen.
H1 antihistamines of the newer generation are the therapy
of first choice (if a standard dose is not effective increased doses up to
fourfold, off-label, should be tried). Whether the prophylactic administration
of H1 antihistamine can suppress potentially life-threatening systemic symptoms
has not yet been investigated. Therefore, patients with severe cold urticaria
should be urgently advised to avoid the triggers and receive an emergency kit
including an epinephrine autoinjector.
Tolerance induction by increasing cold exposure (multiple
daily showers) can be successful, but is not harmless and usually not
permanently practicable.
Contact Urticaria
Contact urticaria is
characterized by a wheal-and-flare response that occurs within 30 to 60 minutes
after contact with intact skin or mucosa to certain agents, but
contact erythema and even burning and stinging without erythema are sometimes
embraced in the definition. Percutaneous or mucosal penetration of the urticant
may have distant effects, including acute urticaria or even anaphylaxis. There
are nonimmunologic and immunologic forms.

Stages of progression in contact urticaria
|
Stage |
Description |
|
1 |
Localized
reaction (redness and swelling) with nonspecific symptoms (burning, itching,
tingling) |
|
2 |
Generalized
reaction |
|
3 |
Extracutaneous
symptoms (rhinoconjunctivitis, orolaryngeal and gastrointestinal dysfunction) |
|
4 |
Anaphylactic shock |
Pathophysiology of
contact urticaria
Nonimmunological contact urticaria
is the most common type
and most benign occurring without prior exposure to
an eliciting substance. Percutaneous microinjection of histamine, acetylcholine, and/or
serotonin by plants (e.g. nettle stings) or
animals (e.g. caterpillars, jellyfish) as well as contact with
histamine liberators that degranulate mast cells (e.g. dimethyl sulfoxide, cobalt
chloride) can result in contact urticaria. A
more common form is from exposure to either sorbic acid and benzoic acid in eye solutions
and foods such as tomato ketchup or
cinnamic aldehyde and balsam of Peru in
cosmetics; the reaction is mediated by prostaglandin
D2 formation in the epidermis rather than histamine release from the
mast cells, so there is lack of response to antihistamines and the positive
response to non-steroidal anti-inflammatory drugs (NSAIDS). An occupational exposure includes ammonium
per sulphate in hairdressing.
The reaction may take up to 45 min
to develop and remain up to 24 hours. This type of urticaria generally does not
go beyond the localized reaction described in Stage 1, presenting with redness
and swelling along with nonspecific symptoms of burning and itching.
The release of histamine is the
major mechanism of action seen in immunological urticaria. The pathophysiology
of immunological CU differs from nonimmunological CU, as it occurs due to the
production of allergen-specific IgE following prior sensitization to a
causative agent. After the initial binding of allergen-bound IgE to mast cells,
histamine is released resulting in an immediate, localized weal and flare
resolving within 2 h, and progress to generalized urticaria, or even
anaphylaxis if the individual is extremely hypersensitive.
Allergic contact urticaria can be seen in children with atopic
dermatitis who become sensitized to environmental allergens. The commonest causes are foods (for example, nuts, fish,
fruits) or latex. Latex is present as latex proteins in rubber agents such as
gloves, condoms, and urinary catheters. Thus, occupations with the maximum
exposure to latex products are more likely to develop immunological CU,
including healthcare or dental workers.
The oral allergy syndrome is a form
of allergic contact urticaria that presents with itching and mild swelling of
the mouth (lips, tongue, palate and throat), sometimes
associated with other allergic features such as rhino conjunctivitis and
asthma, within minutes of eating fresh
fruits such as apples, pears, peaches and cherries, but not cooked, dried,
peeled or bottled fruit. It usually occurs in hay-fever sufferers and
represents a cross-reaction between pan allergens in grass or birch pollens
with fruit proteins. Angioedema and anaphylaxis are fortunately very rare.
Oral allergy syndrome may respond to
antihistamines or to a sympathomimetic agent such as ephedrine taken by mouth.
Treatment of contact
urticaria
Emphasis for treatment of CU should
be placed on prevention–thorough history taking and appropriate clinical
testing will help determine the problematic materials. Once the diagnosis of
contact urticaria is made, avoidance is almost always possible. In case of
contact, patients should carry antihistamines and receive education on
self-administration of subcutaneous epinephrine.
Because contact with an eliciting
substance may still occur, management is divided into first-, second-, and
third-line therapies. In addition to patient education, first-line therapy
includes the use of H1 receptor antihistamines. The ability of these agents to
suppress the histamine-induced wheal-and-flare response has been well studied
in urticaria they may decrease both the number and the duration of wheals. H2
receptor antagonists, including ranitidine and famotidine, are often used along
with H1 receptor antagonists, because 15% of the skin receptors are of the H2
type. The improved tolerability of newer, nonsedating antihistamines may give
them a clear advantage over older antihistamines and corticosteroids.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS OF URTICARIA
The
differential diagnosis of urticaria includes all dermatologic conditions with
an urticarial component, including insect bite reactions (popular urticaria),
pre-bullous phase of pemphigoid (i.e. urticarial pemphigoid), acute eyelid
contact dermatitis (versus angioedema), urticarial drug reactions (e.g.
antibiotics), and the urtication that may occur when lesions of urticaria pigmentosa
are rubbed. In all these conditions, the urticarial component is part of a more
prolonged inflammatory process (or mast cell proliferation in the case of
mastocytosis) than in true urticaria and should be readily distinguishable by
the prolonged duration of individual lesions. Especially in young children,
urticaria may develop a dusky center and be confused with erythema multiforme.
Diagnosis
Clinical history taking and diagnosis
A comprehensive history is essential in every
patient with urticaria. It should cover the duration of disease, frequency of
attacks, duration of individual lesions, associated illness, previous
treatment, known adverse reactions, past and family history, occupation and
leisure activities, and an assessment of the impact of the disease on the
patient’s quality of life. A full physical examination looking for the
morphology and duration (by circling individual lesions) of wheals, purpura,
and signs of systemic disease should always be undertaken, but it is often
normal. Weals
lasting more than 24–48 h, particularly if painful or tender, suggest the
possibility of urticarial vasculitis or delayed pressure urticaria, but can
occur in spontaneous urticaria. Purpura, although rarely seen, suggests
urticarial vasculitis, but can occur in spontaneous urticaria in severe cases. The occurrence of angioedema should be noted,
particularly if it has affected the oropharynx with difficulty in swallowing or
breathing. Enquiry should be made for systemic symptoms sometimes associated
with cutaneous lesions, including malaise, headache, abdominal pain,
arthralgia, wheezing and syncope. Possible precipitating or aggravating
factors—including physical factors such as heat, cold, localized pressure on
the skin, friction and sunlight—should be sought directly. It is important to
ask about any association with recent acute infection, drugs, non-prescription
medicines and foods, although the latter are rarely a cause for chronic
urticaria. A family history of atopy, autoimmunity or angioedema may be useful
information.
Investigation should be targeted at specific
features identified in the clinical assessment, and may include blood tests,
skin biopsy (obtained in all patients with lesions lasting more than 24 hours),
challenges for physical urticarias, food additives and drugs, and, infrequently
as an extended investigation, skin tests for allergy and measurement of
histamine-releasing auto antibodies. Most patients with
antihistamine-responsive urticaria do not need an extensive investigation.


Investigation of urticaria
Acute urticaria
Usually none, except where suggested by the history
·
Infection
o Throat swab if
pharyngeal symptoms
o Other appropriate
samples for suspected viral or bacterial infection
·
Drugs
o Withdraw suspected
drugs
·
Foods
o Investigate for IgE
sensitization (skin prick tests or Immuno CAP where appropriate)
Episodic urticaria
-Pseudoallergy challenge capsules (if available)
-Food additives
-Non-steroidal
antiinflammatory drugs
Chronic urticaria
Physical
challenge provocation tests (where suggested by the history)
Blood tests
(spontaneous urticaria, if unresponsive to H1-antihistamines)
FBC,
ESR, thyroid antibodies, thyroid function tests
§ C4 complement (angioedema
without weals)
§ Non‐organ specific auto antibodies
(if associated autoimmune disease possible)
§ Autologous serum skin
test (where facilities are available)
§ Basophil histamine
release assay or basophil activation tests (if functional autoantibodies
suspected)
§ Helicobacter pylori (stool antigen or
urea breath test) (if peptic ulcer symptoms)
§ Stool for ova, cysts
and parasites (foreign travel)
§ Chest X‐ray (if lymphoma
considered)
§ Others: as determined
by the history and physical examination
§ 3‐week trial of a low pseudo
allergen diet
§ Skin biopsy (12–16 h
old lesions, if urticarial vasculitis suspected)
Acute urticaria
IgE-mediated reactions to environmental allergens as a cause of acute urticaria and contact urticaria can be confirmed by skin prick testing and serum radioallergosorbent tests (RAST). Results of both have to be interpreted in the clinical context.
Chronic urticaria
No
investigations are routinely required for the majority of patients with mild
disease that responds to antihistamines. A useful screening profile for
non-responders with more severe disease could include a complete blood count and
erythrocyte sedimentation rate (ESR).
An
elevated ESR suggests the possibility of an underlying systemic disease (lupus
erythematosus, urticarial vasculitis), and an eosinophilia would prompt a
search for parasitic disease. Thyroid function tests and thyroid auto antibodies
should be performed, if indicated clinically, as
around 14% of patients with chronic ordinary urticaria may have thyroid
autoimmunity and may be an indicator of autoimmune
urticaria. Initial reports suggest that treatment with thyroxine to
suppress thyroid activity may resolve the urticaria. Tests for bowel parasites may be
considered in the appropriate clinical setting.
If angioedema is a major component of the disease,
measuring plasma C4 complement should be performed as a screening test for
hereditary or acquired C1 esterase inhibitor deficiency.
A skin biopsy may be helpful if the weals persist for
more than 48 h and do not respond to antihistamines. Urticarial vasculitis or
delayed pressure urticaria is then suspected.
The term “autoimmune” urticaria is increasingly being used
for patients with evidence of functional serum auto antibodies. Demonstration
of autoreactivity in the form of a
localized wheal and flare response to intradermal injection of autologous serum
(the autologous serum skin test; ASST) provides useful evidence of functional
factors in the blood, but is not specifically a test for auto antibodies. A
negative test, however, has very good negative predictive value for the absence
of functional antibodies.
Autologous serum skin test (ASST): At 30 minutes, a red wheal response
is present at the site of an intradermal injection of autologous serum, but not
at that of a normal saline control. For the test to be positive, the wheal
response at the serum injection site must be at least 1.5 mm greater in
diameter than the control site. The ASST is a reasonably sensitive and specific
screening test for functional auto antibodies as detected by the basophil
release assay.
Immunoassays for anti-FcεRI and anti-IgE antibodies (commercially available)
have been detected by Western blot and ELISA. There
is overlap between: (1) autoreactivity; (2) functional
auto antibodies as detected via basophil or mast cell assays; and (3)
immunoassays (“immunoreactivity”). The strongest evidence for an autoimmune
etiology of urticaria is provided by demonstrating all three features, but many
clinicians would accept a positive ASST and/or a positive functional assay as
providing sufficient proof of autoimmunity to guide therapies and prognosis.
Attention should be paid to medication, especially
NSAIDs. Patients frequently suspect allergy to foods, but this is rarely if ever
found in adults with chronic ordinary urticaria. A food diary may be helpful,
especially in episodic urticaria, but it should be remembered that the time
interval may vary from a few seconds with allergy and up to 24 h with dietary
pseudo allergens, and the substance may have been consumed regularly for years.
If the patient suspects food additives, or if they have improved substantially
on elimination of the substance or on a diet free of food additives, challenge
testing can be carried out on a placebo-controlled basis. This is performed
when the patient is in relative remission, and antihistamine therapy need not
be stopped, although this is desirable. The most important test substances are
tartrazine (E102), aspirin, sodium benzoate (E211) and 4-hydroxybenzoate
(E214–219). The patient records any urticarial response, and if present the
suspected substance should be re-administered on at least one occasion for
confirmation of the results. When the provocation tests are positive, a
tartrazine-free, salicylate-free or other appropriate diet can be suggested and
is usually only necessary for a few months. It is usually inappropriate to
carry out provocation tests in patients who respond well to antihistamines. A
low-pseudo allergen diet may be helpful for some patients, especially if
antihistamines have failed or are not accepted.
MANAGEMENT OF URTICARIA


Patients should be given advice and
information on common precipitants, treatments, and prognosis. Non-specific measures including the wearing of loose
fitting clothing and application of soothing creams with menthol may be
helpful. Patients should minimize aggravating factors including overheating,
stress and alcohol. Aspirin and aspirin-containing compounds,
other NSAIDs, and also opiates, should be avoided if possible. Paracetamol is
usually a satisfactory alternative. Selective COX-2 inhibitors may be tolerated
by aspirin sensitive patients if an antiinflammatory drug is essential. If food
additives, colorings or preservatives have been proven to be a problem, diets
excluding these substances may be of value to a limited number of patients.
Drug therapies can be first, second, or third-line.
First-line therapies (antihistamines)
Histamine is the main mediator of urticaria, with
H1-receptor activation causing itch, wealing and flare, while H2 activation
plays a smaller role in weal formation. Thus, H1 antihistamines are the
first-line treatment for all types of urticaria,
although not all patients will respond and only about 40% will clear or almost
clear at licensed doses. Antihistamines reduce pruritus, flatten wheals,
shorten wheal duration and reduce wheal numbers, even though they may not clear
urticaria completely. It is worth discussing the relative benefit with patients
who feel that “they haven’t worked”. Generally H1 antihistamines are
rapidly absorbed, reaching peak serum concentrations in 1–3 h.
Antihistamines should be taken on a daily
basis, the frequency depending on their half-life. In other words, they should
not be taken only when the patient is symptomatic. As a general rule,
antihistamines are safe and have few significant adverse effects. They can be
grouped into first-generation (classic) antihistamines, second-generation (non-
or minimally sedating) antihistamines and their derivatives, and the H2 antagonists.
Classical
antihistamines
The use of classical antihistamines is limited by their
side effects, including sedation, anticholinergic properties and paradoxical
excitation in children. However,
in combination with a daytime non-sedating antihistamine, they can be taken at
night if sleep is disturbed by urticaria, but the following day they may
interfere with skilled tasks (e.g. operating machinery and driving) or reduce
the ability to concentrate at work or school and patients should be
warned of this. Hydroxyzine is the most potent of the classical antihistamines.
25 mg of hydroxyzine is equivalent to 10 mg of cetirizine.
Second-generation antihistamines
The second generation of potent, specific, low-sedation H1
antihistamines is now the treatment of choice. They are
usually well tolerated, with the majority of patients requiring only once-daily
oral dosing. Their main advantage is low sedation at doses recommended
by the manufacturer and minimal anticholinergic side effects, although an
occasional individual may develop sedation with any of them. They are at least
as effective as hydroxyzine and generally as effective as each other. There is
no clear evidence that tolerance occurs after continued use. Very rarely,
antihistamines appear to make urticaria worse, particularly with cetirizine. A European consensus paper has
recommended increasing the daily dose of second-generation H1
antihistamines up to fourfold for difficult urticaria. It is possible that
their additional anti-allergic and anti-inflammatory properties may be
clinically beneficial at these higher doses.
Cetirizine (adult dose 10 mg/day) is poorly metabolized
in the liver and is excreted, predominantly in the urine, unchanged. It is also
rapidly absorbed and may cause sedation and is best taken at night. Cetirizine
reduces dermal eosinophil cell accumulation in vitro and in vivo. However, the
clinical importance of this effect in the treatment of delayed pressure urticaria
and urticarial vasculitis, where eosinophils may be an important component of
the inflammatory cell infiltrate, is uncertain.
Fexofenadine is licensed for urticaria at
180 mg daily. It is the active metabolite of terfenadine, but does not appear to
have the potential for ventricular arrhythmias of its parent drug at licensed
doses
and has the widest therapeutic window of the second generation antihistamines.
Loratadine (adult dose 10 mg daily) is a derivative of
azatadine. Although loratadine is also metabolized in the liver by cytochrome
P450 to some extent, so far no clinically proven, relevant drug interactions
have been reported.
Desloratadine (an active metabolite of
loratadine) and levocetirizine (the active enantiomer of cetirizine) probably
offer no clinical advantage over their parent drugs at equivalent doses.
Low-sedation antihistamines are used to reduce urticarial
activity, with minimal side effects. Individual response is variable, but
adequate dose and timing in relationship to maximal urticarial activity is
important. Alternative low-sedation antihistamines can be tried, and sedating
ones added at night. A combination of an H1 antihistamine with an H2 antagonist
may be more effective than H1 antihistamines alone in some patients. Use of
ranitidine (adults 150 mg twice a day) is preferable to cimetidine, which has
more antiandrogenic side effects and potential drug interactions.
Adverse effects of
antihistamines
Sedation is the
major risk of classical antihistamines and may be seen in some patients with
second‐generation antihistamines, particularly at above licensed
doses. Concerns
about the potential cardiotoxity of antihistamines have receded since
terfenadine and astemizole have been withdrawn from the market. The classical antihistamines
hydroxyzine and diphenhydramine also have the ability to induce Q–T
prolongation, emphasizing that higher than recommended doses of these
antihistamines should be used only with caution.
Antihistamines in
pregnancy
Antihistamines cross the placenta. They should be avoided
in pregnancy and particularly in the first trimester if possible. If it is not
possible, then chlorphenamine appears to be the least risky to use based on its
long availability and safety record. Current guidelines on urticaria support
the use of cetirizine and loratadine beyond the first trimester of pregnancy if
the benefits of an antihistamine are considered to outweigh any risks of
administration for an individual patient.
Antihistamines in childhood
The principles of prescribing of
antihistamines in childhood are the same as for adults. Doses should follow the
relevant manufacturer's recommendations.
Second-line therapies (targeted therapy)
Second-line therapies may be considered when urticaria does
not respond well to antihistamines. They should usually be prescribed as
additive therapies (to antihistamines) rather than as alternatives. It is
unusual for children to need second-line therapies, except the occasional use
of prednisolone for very severe acute exacerbations of chronic urticaria.
Oral corticosteroids are effective in severe urticaria
when started at high doses, such as 0.5–1.0 mg prednisolone/kg/day. It should be considered primarily for the short-term
management of “crisis” urticaria and serious angioedema of the throat as a
rescue medication, when, often, a single dose or
several daily doses will be sufficient to re-establish control with regular
full-dose antihistamines. Although short courses are useful for acute
exacerbations, prolonged use should be avoided because of the risk of side
effects. Rebound is also a common problem and
the long-term course of the urticaria is often not altered. Oral corticosteroids
are often required for disease control in severe delayed pressure urticaria and
urticarial vasculitis, but every attempt should be made to minimize the dose
and duration.
Epinephrine
(adrenaline) by subcutaneous or intramuscular injection is the treatment of
choice for anaphylactic shock or severe anaphylactoid reactions whether due
to an allergy, pseudo allergy, or physical urticaria. Epinephrine may also be
necessary for angioedema of the oropharynx in severe acute allergic urticaria
and idiopathic angioedema, but it is rarely required for chronic urticaria and
is not effective for HAE.
It acts rapidly by vasoconstriction and stabilizing mast cells through
β-adrenoceptor stimulation. Directing epinephrine
mist from an aerosol inhaler onto mucosal angioedema may be helpful for minor
episodes, but for severe reactions, particularly of the anaphylactic
type, epinephrine must be injected intramuscularly. Treatment should be
repeated if there is no improvement after 10–15 min. Side effects of epinephrine includes tachycardia, anxiety
and headache. It should be used with caution in patients with hypertension,
ischemic heart disease, cerebrovascular disease and diabetes mellitus.
Coadministration of tricyclic antidepressants (including doxepin) and
β-blockers should be avoided. For reassurance, patients who are prone to severe
acute allergic urticaria and idiopathic angioedema may carry at least two unexpired self-administered
epinephrine ‘pens’ and they need to be aware of side effects, drug interactions
and potential rebound phenomenon.
The choice of other
second-line therapies will be influenced by the clinical situation.
Perhaps the most
promising new class of drugs is the leukotriene
receptor antagonists, which have been shown to benefit aspirin-sensitive
urticaria and may be of value in delayed pressure urticaria and autoimmune
urticaria when added to antihistamines.
Thyroxine appears to reduce urticarial activity in
some clinically euthyroid patients with
elevated levels of antithyroid auto antibodies. Sulphasalazine
and dapsone
may be useful for delayed pressure urticaria, especially when oral
corticosteroids are otherwise required for disease control.
Third-line therapies (immunomodulatory)
Some patients with severe urticaria unresponsive to
antihistamines have an autoimmune etiology and they are treated with immunomodulators.
Cyclosporine
(3–4 mg/kg/day) for
1–3 months appears to clear or substantially
benefit approximately two-thirds of patients with chronic autoimmune urticaria
refractory to antihistamines. However, only 25% of responders remained clear or
almost clear 4–5 months after discontinuing therapy, and symptomatic side
effects (e.g. gastrointestinal) were common.
Other immunosuppressive therapies, including
methotrexate, mycophenolate mofetil, azathioprine and cyclophosphamide, may
work for some patients with severe chronic urticaria, if cyclosporine fails.
Fourth line treatment
Omalizumab (OM) (humanized anti-IgE monoclonal antibody) has shown very
good results in H1 antihistamine unresponsive spontaneous and
inducible urticarias. The recommended dose of OM is 300mg by
subcutaneous administration every 4 weeks
and around 65% of patients experience a complete or almost complete response.
Most patients experience flare up if administration of OM is delayed by > 30
days. Although OM has a significant effect on urticarial symptoms, patients response patterns
vary; fast responders experience a response within 2-4 weeks after initiating
treatment, while some patients experience a slower response, which is seen
12-16 weeks after initiation of treatment. Therefore, it is recommended that OM
treatment is continued for at least 6 months before considering other options.
Relapse of urticarial symptoms is often seen 2-8 weeks after the last injection
of OM; in such cases, retreatment with OM has obtained good results. The most
commonly reported adverse effects with OM are headache, injection site itch and
redness and nausea. No severe adverse effects or a complication to OM has been
reported.
The updated version of the European Academy of
Allergology and Clinical Immunology (EAACI), the EU-founded network of excellence,
the Global Allergy and Asthma European Network (GA2LEN), the European
Dermatology Forum (EDF), and the World Allergy Organization (WAO) [EAACI/GA²LEN/EDF/WAO]
urticaria guideline published in early 2018 contains new aspects regarding the
diagnosis and treatment of patients with chronic urticaria.
Chronic
urticaria is a common disease, with a prevalence of at least 1 %. It is
defined by the presence of pruritic wheals, angioedema or both for a
period lasting more than six weeks.
With
chronic urticaria, a distinction is made between chronic spontaneous urticaria
(CSU) and chronic inducible urticaria (CIndU). The former is characterized by
spontaneous symptoms that are not associated with a specific trigger. The
latter, on the other hand, requires specific triggers for the urticarial
symptoms to occur, such as sunlight, pressure, friction, or exposure to heat or
cold (Table).
While CSU is two to three times more common than CIndU, many patients have more
than one type of chronic urticaria. Chronic urticaria can have a significant
impact on quality of life; it is associated with depression and anxiety
disorders and interferes with the patient's performance in everyday life, at
school and at the workplace. It is therefore crucial to provide chronic urticaria
patients with the best treatment possible, that is, to attempt to achieve
complete symptom control and taking into consideration
as much as possible the safety of treatment and the quality of life of each
individual patient.
In
the vast majority of patients, this goal can be achieved with the treatment
options and tools for measuring disease activity and control available today.
Classification of
chronic urticaria
The
classification of urticaria is based on its duration as acute (≤ 6 weeks) or
chronic length (> 6 weeks) and as inducible (specific eliciting factor such
as cold, heat or sunlight involved) or spontaneous (no specific eliciting
factor involved). Spontaneous urticaria (also referred to as idiopathic
urticaria) and inducible urticaria (also referred to as physical urticarial)
often co-exist in patients.
Table
|
Chronic urticaria |
||
|
Spontaneous
urticaria (CSU) |
Inducible
urticaria (CIndU) |
|
|
known cause |
unknown cause |
|
Pathogenesis of urticaria and clinical
presentation
The
wheals and angioedema associated with chronic urticaria are caused by active
and degranulating mast cells. Mast cell mediators such as histamine lead to
vasodilatation and increased permeability, with subsequent edema in the upper
dermis (wheals) and/or deep dermis and subcutis (angioedema). More than half of
all CSU patients develop wheals and angioedema; up to one‐third of CSU patients show wheals
but no angioedema; and about one in ten CSU patients solely experiences
angioedema but no wheals.
Based
on what we know today, cutaneous mast cell degranulation in patients with
chronic urticaria involves autoimmune mechanisms.

Type I and IIb autoimmune mechanisms of
mast cell activation in patients with CSU.

Two
different mechanisms are thought to be involved in CSU. In type 1 autoimmune
CSU, IgE auto antibodies bind to the high‐affinity (cutaneous) mast cell receptor. Degranulation and mediator release occurs after auto-allergen cross‐linking (endogenous allergens
recognized and bound by IgE). Common CSU‐associated auto-allergens identified to date include thyroid
peroxidase and interleukin 24.
In
type IIb autoimmune CSU, mast cell degranulation and mediator release is caused by IgG auto antibodies directed against the high‐affinity IgE receptor or IgE molecule. The definitive diagnosis of type IIb autoimmune
urticaria is based on a positive autologous serum test, a positive basophil
histamine release test, and evidence of these auto antibodies, for example by
means of ELISA. The mechanisms involved in mast cell degranulation in CIndU
have been less well investigated. Here, too, it is postulated that autoimmune
mechanisms are responsible for cutaneous mast cell degranulation.
The
reaction of mast cells to degranulators is modulated by many different signals.
The most important mast cell modulators in CSU include neuropeptides, complement
factors, pathogen‐associated
factors as well as foods and drugs in patients intolerant to the latter two.
The presence and effects of one or more of these modulators, for example in
case of mental stress or chronic infections, may explain their role in the
pathogenesis and disease activity in patients with CSU. This also applies to
the improvement in some patients following the avoidance of certain
foods or the treatment of chronic infections.
Diagnostic approach to chronic spontaneous
urticaria
The
current version of the EAACI/GA²LEN/EDF/WAO urticaria guideline recommends the
following diagnostic approach in patients with CSU: (1) Rule out differential
diagnoses, (2) Rule out severe inflammatory diseases, and (3) measurement of
disease activity and control.
Important
differential diagnoses of CSU include auto-inflammatory syndromes such as
Schnitzler syndrome and urticarial vasculitis (Figure). While these two
disorders are likewise characterized by wheals, unlike CSU, these are mediated
by interleukin 1 and not by histamine. It is therefore important to identify
these differential diagnoses in order to initiate effective treatment. Besides
chronic urticaria, recurrent angioedema without wheals also occurs in patients
with bradykinin‐mediated
forms of angioedema such as angiotensin‐converting enzyme (ACE) inhibitor‐induced angioedema and hereditary
angioedema (Figure). In these cases, the swelling is caused by bradykinin and
does not respond to classic drugs used for urticaria.
Figure

Diagnostic algorithm for patients with
urticaria, angioedema or both. Abbr.: AAE,
acquired angioedema with C1 inhibitor deficiency; ACE inhibitor, angiotensin‐converting enzyme inhibitor; AIS,
auto-inflammatory syndrome; HAE, hereditary angioedema.
Once
the diagnosis of chronic urticaria has been confirmed, it is important to
determine which form or forms of chronic urticaria the patient has, whether
they can deliberately trigger wheals or angioedema. While patients affected by
the various forms of CIndU are able to do so, individuals with CSU are not.
The
guideline recommends a two‐step
approach with respect to laboratory tests for patients with CSU. In all CSU
patients, initial tests should include C‐reactive protein levels and/or erythrocyte sedimentation rate
as well as a differential blood count. While the goal of these tests is to rule
out systemic inflammatory events, the urticaria itself may lead to elevated
inflammatory markers, too. Depending on the history as well as on the duration
and severity of chronic urticaria, patients should subsequently undergo further
diagnostic workup for causes and associated disorders, including autoimmune
diseases, infections and intolerances.
For
patients with CSU, the guideline recommends measurement of disease activity,
disease burden and disease control using standardized tools. This enables the
physician to accurately assess disease severity and course, including treatment
success. The current guideline endorses the urticaria activity score
(UAS) and/or the angioedema activity score (AAS) to assess disease
activity in CSU patients. In order to calculate the UAS, patients record and
quantify their symptoms (wheals and pruritus) on a daily basis in a diary. The Angioedema Activity Score (AAS) is also a patient's
self-reported evaluation of the activity of angioedema, which includes scoring
of five key factors (duration, physical discomfort, impact on daily activities,
impact on appearance, and overall severity) from 0 to 3 of each, respectively
(thus a daily score of 0–15).
Urticaria Activity Score 7 scoring criteria for chronic
spontaneous urticaria disease activity

Besides
disease activity, it is also useful and recommended to assess quality‐of‐life impairment. In everyday clinical practice, assessment
of disease activity as well as of quality‐of‐life
impairment disease burden facilitates treatment decision making, especially
prior to employing systemic therapies.
Diagnostic approach to chronic inducible
urticaria
If
CIndU is suspected, (1) differential diagnoses should be ruled out, (2) the
diagnosis should be confirmed by provocation tests, (3) disease activity should
be measured by determining the trigger threshold, and (4) disease burden and
control should be measured.
Differential
diagnoses are ruled out by taking a thorough medical history, and possibly by
subsequent diagnostic tests (Figure). Provocation tests are conducted to
confirm the diagnosis in all forms of CIndU. In this context, it should be
noted that a patient may have multiple forms of CIndU and should therefore be
tested accordingly as suggested by his/her history. When performing provocation
tests, it should be borne in mind that these tests are affected by symptomatic
therapies such as antihistamines. Treatment should therefore be interrupted at
least three – ideally seven – days prior to testing. If this is not possible,
the test result should be evaluated with caution. Provocation tests, just as
determination of the trigger threshold, should be conducted prior to treatment
initiation and during follow‐up.
To improve comparability of test results, standardized provocation test
procedures should be used.
Treatment of chronic urticaria
Treatment
of chronic urticaria follows a standard approach with the goal of achieving
complete freedom from symptoms. All patients should avoid known triggers. In
particular, this includes certain medications such as non steroidal antiinflammatory
drugs and relevant triggering stimuli in the case of CIndU. However, given that
this approach results in freedom from symptoms in only very few cases,
symptomatic treatment is recommended for nearly all patients, and should be
based on the new treatment algorithm.

Recommended treatment
algorithm for chronic urticaria. nsAH: non‐sedating
antihistamine
Second‐generation H1 antihistamines remain
the treatment of choice. Unlike first‐generation antihistamines, which should no longer be used,
they have hardly any or only mild sedative effects. Initially, antihistamines
shall be administered at the approved dose. It is important to instruct
patients that antihistamines must be taken on a daily basis and not on demand.
About 40-50%
of patients with CSU will not respond to standard doses of H1-antihistamines.
If
continuous treatment for 2–4 weeks does not lead to adequate control of
symptoms, the guideline recommends up dosing (up to four times the standard
dose). Although using a higher‐than‐approved dose constitutes off‐label treatment, it is much more
effective than standard‐dose
therapy and has a similar side effect profile.
The guideline
states that the majority of patients with urticaria not responding to standard
doses will benefit from up-dosing of the second-generation H1-antihistamine and
highlights studies that have documented the benefit of using up to fourfold
higher than licensed doses of cetirizine, desloratadine, fexofenadine,
levocetirizine, bilastine, ebastine, and rupatadine.
In contrast to
the previous guidelines, and because of insufficient evidence in the
literature, this recent guideline does not recommend adding another
second-generation H1-antihistamine, a H2-antagonist, a leukotriene receptor
antagonist or a first-generation H1-antihistamine at bedtime as next steps in
treatment of antihistamine resistant cases of chronic urticaria.
Although many patients
respond to up-dosing with second-generation H1-antihistamines, around half of
chronic urticaria patients will not achieve satisfactory control with
antihistamine treatment - even at four times the standard dose. For such
patients, the guideline recommends adding omalizumab to the second-generation
H1-antihistamine.
If
sufficient improvement does not occur after 2–4 weeks of second‐generation antihistamine therapy at
a higher‐than‐standard dose, omalizumab should be
added to the regimen. A recombinant humanized anti‐IgE antibody, omalizumab is
administered by subcutaneous injection at the recommended dose of 300 mg
every four weeks. It is approved for the treatment of chronic spontaneous
urticaria in patients 12 years and older. Most patients show a – usually
complete – response even before the second dose. A small percentage of patients
require multiple doses to achieve treatment success. Omalizumab has also been
shown to be effective and safe in the treatment of CIndU patients. It is particularly effective in the treatment of cholinergic
urticaria, cold urticaria, solar urticaria, heat urticaria, symptomatic
dermographism, and delayed pressure urticaria but it is not FDA approved for
treatment of any inducible urticaria. In CSU, omalizumab has been shown to
prevent angioedema development, improve quality of life, be suitable for
long-term treatment and effectively treat relapse after discontinuation. Dosing
of omalizumab in CU is independent of total serum IgE.
If
there is no success after six months of omalizumab therapy, off‐label treatment with cyclosporine is
recommended.
The use of
systemic corticosteroids in the treatment of chronic urticaria is generally to
be avoided. Long term use of systemic steroids is definitely not recommended
because of the myriad of associated side effects, but the 2017 guideline
suggests that a short course of oral corticosteroids - up to 10 days — may be
helpful in reducing disease duration/activity in acute urticaria or
exacerbations of CSU.
Comparison among
pharmacotherapies in refractory chronic urticaria patients who are resistant to
high dose or combination antihistamine therapy

Patients with comorbidities
