Key notes
·
Cutaneous
fungal infections are broadly divided into two groups: (1) those that are
limited to the stratum corneum, hair, and nails; and (2) those that involve the
dermis and subcutaneous tissues
·
Superficial
fungal infections of the skin are most often due to dermatophytes and Candida spp.
·
“Subcutaneous”
mycoses are often the result of implantation, while systemic or “deep” mycoses
of the skin usually represent hematogenous spread or extension from underlying
structures
·
In
the immunocompromised host, opportunistic fungi, e.g. Aspergillus and Mucor spp., can
lead to both cutaneous and systemic infections
|
ORGANIZATION OF
CUTANEOUS MYCOSES |
|
|
Superficial |
Involve stratum corneum, hair, or
nails |
|
Subcutaneous |
Involve dermis or subcutaneous
tissue |
|
Systemic (“deep”) |
Involve dermis or subcutaneous
tissue |
|
“True” pathogens |
Skin involvement usually reflects
hematogenous spread or extension from underlying structures |
|
Opportunistic |
Primary or secondary skin lesions
in immunocompromised hosts |
Superficial Mycoses
Superficial fungal
infections are the most common mucocutaneous infections, often caused by an
imbalanced overgrowth of mucocutaneous microbiome. Superficial mycoses are due
to fungi that only invade fully keratinized tissues, i.e. stratum corneum,
hair, and nails. They can be further subdivided into those that induce minimal,
if any, inflammatory response, e.g. tinea (pityriasis) versicolor, and those
that lead to more substantial cutaneous inflammation, e.g. dermatophytoses.
Candida species require a warm humid environment whereas Malassezia species
require lipids for growth.
|
SUPERFICIAL MYCOSES OF THE
SKIN |
||
|
Cutaneous disorder |
Pathogen(s) |
|
|
Minimal, if any, inflammation |
Tinea (pityriasis versicolor) |
Malassezia furfur, M. globosa |
|
Inflammatory response common |
Tinea capitis, barbae, faciei, corporis, cruris,
manuum, pedis |
Trichophyton, Microsporum, Epidermophyton spp. |
|
Cutaneous candidiasis |
Candida albicans,
other Candida spp. |
|
Dermatophytoses
Salient features
·
Dermatophyte
causes infection of keratinized tissues including skin, hair, and nails.
·
Dermatophyte
species are contained in 3 genera (Epidermophyton, Microsporum,
and Trichophyton), which are further divided according to 3 natural
habitats (humans, animals, and soil).
·
Trichophyton is the most common genera isolated.
·
Trichophyton rubrum is the most common cause of
dermatophytosis of the skin.
·
Trichophyton tonsurans is the most common cause of
tinea capitis.
·
Onychomycosis
is the name given to dermatophytosis of the nails.
·
Microscopic
examination, culture, Wood light evaluation, and histopathology may all be
useful in confirming diagnosis.
·
Several
topical and oral antifungals are available for effective treatment of
dermatophytosis.
·
Infections
involving hair bearing skin and nails typically require oral treatment.
Introduction
Dermatophytes are a group of fungi that have the unique
ability to invade and multiply within the nonviable keratinized cutaneous
structures including stratum corneum, nails, and hair. Arthrospores can survive
in human scales for 12 months. Dermatophytosis denotes an infection caused by
dermatophytes.
Glossary of Terms:
Anthropophilic—preferring
humans over other animals as natural habitat
Geophilic—preferring
the soil over humans and animals as natural habitat
Zoophilic—preferring animals over humans as natural habitat
Hyphae—long,
filamentous fungus cells forming a branching network called mycelium
Arthroconidia—asexual
spore produced by segmentation of hyphae
Macroconidia—asexual
large multinucleate spores produced by vegetative reproduction
Microconidia—asexual
small spores produced by vegetative reproduction
Dematiaceous—melanin
in the cell walls of its conidia, hyphae, or both results in a darkly colored
fungus
Ectothrix—dermatophyte
growth pattern with spores forming a sheath on the outside of the hair shaft
Endothrix—dermatophyte
growth pattern with spore formation within the hair shaft
Favus—dermatophyte
growth pattern with hyphae and air spaces within the hair shaft
|
TYPES OF DERMATOPHYTES BASED ON MODE OF
TRANSMISSION |
||
|
Category |
Mode of transmission |
Typical clinical features |
|
Anthropophilic |
Human to human by fomites, or by direct skin-to-skin
contact |
Mild to non-inflammatory, chronic |
|
Zoophilic |
Animal to human by fomites, or by direct
skin-to-skin contact |
Intense inflammation (pustules and
vesicles possible), acute |
|
Geophilic |
Soil to human |
Moderate inflammation |
Morphology:
Morphology in lesion, dermatophytes
appears as hyphae and arthrospores. In cultures on sabouraud’s agar, they form
characteristic colonies consisting of septate hyphae and two types of asexual
spores, microconidia and macroconidia. Differentiation into the three genera is
based mainly on the nature of macroconidia.
Trichophyton: infects skin, hair
& nails,
Microsporum: infects skin & hair
but not nails,
Epidermophyton: infects skin &
nails but not hair
PATHOGENESIS OF DERMATOPHYTES
Dermatophyte infections involve three
main steps:
1- Adherence to keratinocytes,
2- Penetration through and between
cells,
3- Development of a
host response.
Dermatophytes produce
keratinases (enzymes that break down keratin), which allow adherence and
invasion of the fungi into the stratum corneum of skin, hair, and nails, and
also to utilize keratin as a source of nutrients for survival. If invasion is
successful, clinical disease occurs. As a consequence of keratin degradation, fungal metabolic products diffuse through malphigian layer and the host
develops an inflammatory response with subsequent release of pro-inflammatory
mediators.
Adherence
The
first stage of infection involves contact with and adherence of the infectious
elements of the fungus (arthroconidia), asexual spores formed by fragmentation
of hyphae, to the surface of keratinized tissues. The
ability of certain fungi to adhere to a particular host arises from a
variety of microbial mechanisms and host factors. Following several
hours of successful adherence, the spores begin to germinate and prepare for
the next step, invasion.
Invasion/Penetration
Trauma and maceration facilitate
penetration of dermatophytes through the skin. Invasion of germinating fungal
elements is further accomplished through secretion of specific proteases,
lipases and ceramidases, the digestive products of which also serve as fungal
nutrients. Once dermatophytes have invaded
(penetration through and between cells) and begun to proliferate in the skin,
several mechanisms aid in limiting the infection to dead keratinized tissue. Although the inflammatory responses of ringworm infection
involve the Malpighian stratum of the epidermis and the dermis, the fungus
itself is found growing only within the stratum corneum of the epidermis,
within and around the fully keratinized hair shaft, and in the nail plate and
keratinized nail bed. Within these keratinized tissues, the fungus exists only
as mycelium and arthroconidia. Fungal mannans in the cell wall of dermatophytes may
decrease the rate of keratinocyte proliferation, thereby reducing
the likelihood of the fungus being sloughed off prior to invasion. This
mechanism is thought to contribute to the chronicity of infections caused
by T. rubrum.
Host Response
Defense against the fungi causing
ringworm depends on both innate and acquired immune mechanisms. Serum factors
such as unsaturated transferrin, inhibiting the growth of dermatophytes by
binding to the hyphae. Another important mode of defense is provided by the presence
of fatty acids from sebaceous glands, which inhibit dermatophyte growth in
vitro. It has been postulated that their presence on the skin in
postpubertal children may account for the spontaneous resolution of tinea
capitis after this age, and the rarity of new infections in adults. keratinocytes
response to invading fungal elements by increasing their proliferation
resulting in increased shedding of the fungus as well as secretion of
antimicrobial peptides including human β defensin-2 as well as several
pro-inflammatory cytokines. These antimicrobial peptides are known to have activity against bacteria,
viruses and fungi and to play a key role in protection against skin infections
including dermatophytes as well as Candida albicans. The production of
cytokines, such as interleukin 1 (IL‐1), by keratinocytes is important in the mobilization of
neutrophil defenses. It has been shown that neutrophils, and to a lesser extent
monocytes, can kill dermatophyte conidia. It has also been found that
dermatophytes are chemotactic and that they can activate the alternative
pathway of complement activation.
The degree of host inflammatory
reaction depends not only on the host's immune status but also on the natural
habitat of the dermatophyte species involved. Interestingly, anthropophilic
dermatophytes induce secretion of a limited cytokine profile from keratinocytes
in vitro compared to zoophilic species. This difference may reflect the
augmented inflammatory response generally observed with zoophilic species.
The next level of
host defense is cell-mediated immunity resulting in a specific delayed type
hypersensitivity response against invading fungi. It is hypothesized that
dermatophyte antigen is then processed by epidermal langerhans cells and
presented in local lymph nodes to T lymphocytes. The T lymphocytes undergo
clonal proliferation and migrate to the infected site to attack the
fungus. Soon, the fungus is cleared, and
the lesion spontaneously resolves.
Defective cell-mediated immunity may result in chronic or
recurrent dermatophytoses.

Pathophysiology
The clinical appearances of the
various forms of ringworm infection are the result of the combination of direct
damage to the keratinized tissues by the fungus (this applies mainly in hair
and nail infections) and of the inflammatory host response. The latter varies
widely. At one extreme there is the simple hyperkeratosis seen, for instance,
in dry‐type T.
rubrum infections; at the other is the pustular, highly inflammatory kerion
seen most frequently in zoophilic infections.
In classic annular ringworm, the rim
of the lesion shows marked inflammatory changes. By contrast, central zone shows
less inflammation, possibly following elimination of the fungus in the central
zone in stratum corneum. Through the persistence of immunological surveillance,
previously infected skin remains free of fungal hyphae compared with uninfected
skin, and fungal growth proceeds centrifugally. The epidermal turnover rate is
normal within the ring, but more than four times as rapid in the zone where
inflammation is maximal.
Clinical Infection by Structure Involved.
The
pathogenesis of epidermomycosis (A) and trichomycosis (B) are different because
they involve different structures leading to different clinical manifestations.

(A) Epidermal dermatophyte infection
In epidermomycosis, dermatophytes (green
dots and lines) within the stratum corneum not only disrupt the horny layer and
thus lead to scaling, but also elicit an inflammatory response (black dots
symbolize inflammatory cells), which may then manifest as erythema, papules,
and vesicles.

(B) Hair follicle dermatophyte infections
Hair
shaft is involved (green dots) resulting in the destruction and breaking off of
the hair. If the dermatophyte infection extends farther down into the hair
follicle, it will elicit a deeper inflammatory response (black dots) and this
manifest as deeper inflammatory nodules, follicular pustulation, and abscess
formation.
Clinical forms of ringworm infection

The traditional division of ringworm
into different syndromes according to the site of the body infected:
·
Tinea corporis
·
Tinea capitis
·
Tinea barbae
·
Tinea faciei
·
Tinea pedis
·
Tinea manuum
·
Tinea cruris
·
Onychomycocis caused by
dermatophytes
·
Steroid‐related tinea
·
Dermatophytide reactions
Tinea corporis
Definition
Tinea
corporis is a dermatophyte infection of the skin of the trunk and limbs, excluding ringworm of specialized sites the hair, nails,
palms, soles and groin. The infection is generally restricted to the stratum
corneum and most commonly affects exposed skin. Terminal
hair in the affected parts may be invaded.
Pathophysiology
Tinea
corporis can result from human-to-human, animal-to-human (often transmitted by
domestic animals) or soil-to-human spread.
In young children infected with Trichophyton rubrum and Epidermophyton
floccosum, half of the infections may come from their parents. Spread from
existing localized infection (e.g. feet, groins, scalp and nails) is also
common. The characteristic annular appearance of ringworm infections results from
centrifugally spreads of infection through the horny layer of the epidermis
from the point of skin invasion, with elimination of the fungus from the center
of the lesion, and the subsequent resolution of the inflammatory host response
at that site. This area usually becomes resistant to reinfection. However, many
lesions lack any tendency to central clearing. The natural history is variable.
Some inflammatory cases of animal infection resolve spontaneously in a few
months, while a typical case of T. rubrum tinea corporis may persist for
years.
Causative
organisms
Any
dermatophyte can potentially cause tinea corporis, but T. rubrum is the
most common pathogen worldwide, followed by T. mentagrophytes.
Clinical
features
There are
multiple clinical presentations of tinea corporis, and they can mimic other
dermatologic conditions. As
with most dermatophyte infections, the extent of inflammation depends on the
causative pathogen and the immune response of the host. Also, because hair
follicles serve as reservoirs for infection, areas of the body with more hair
follicles may be more resistant to treatment.
The site of infection is typically on exposed skin, unless
the infection represents an extension from a pre‐existing infection and in such cases, infection may spread
from the scalp, down the neck on to the upper trunk, or from the groins on to
the buttocks and lower trunk.
The
typical incubation period is 1 to 3 weeks. Characteristic
lesions are circular, usually sharply marginated with a raised edge. There may be single or multiple plaques. The
latter may remain discrete or become confluent. In inflammatory lesions,
pustules or vesicles within
the active border may dominate and even in mild
infections close observation may reveal one or two small pustules. In less
inflammatory infections, scaling is a common. The scales are at the leading edge,
pointing towards normal skin, whereas in pityriasis rosea they tend to point
towards the center of the lesion. Scale may be lessened or absent if topical
corticosteroids have been used (tinea “incognito”). Central resolution,
which is a common feature of tinea corporis, is perhaps more frequent in
inflammatory lesions. The process is often incomplete, and the central skin may
show post inflammatory pigmentation, a change of texture or residual
erythematous dermal nodules.
Clinical variants
Clinical variants of tinea corporis include Majocchi’s
granuloma and tinea imbricata.
Majocchi’s
granuloma: usually caused
by T. rubrum, is characterized by follicular papulopustules or
granulomatous nodules with scale coalescing to form an annular plaque. This
variant is commonly seen on the legs in women who have concomitant tinea pedis
or onychomycosis and become inoculated after shaving. The combination of trauma
and pre-existing fungal disease elsewhere facilitates follicular inoculation of
fungus. It represents a deep dermatophyte folliculitis in which the wall of the
follicle is disrupted.
Tinea imbricate: It
is a geographically restricted form of tinea corporis (Fiji islands & south
East Asia) caused by the
anthropophilic dermatophyte T.
concentricum. The infection begins as an erythematous scaling ring; centrifugal spread follows, but within the
area of central clearing a second wave of scaling soon arises. The process is
repeated to give numerous concentric rings and, as the natural history is
normally prolonged, the whole body may become affected. Pruritus is intense and
may lead to lichenification.
Disease
course and prognosis
Spontaneous
resolution can occur but is uncommon.
Treatment
Localized tinea corporis, especially
of recent origin, commonly responds to topical therapy applied twice daily,
usually for about a month. Topical terbinafine often works in a shorter time
period (e.g. 2 weeks). In more widespread infections of recent onset, oral
terbinafine or itraconazole will generally be preferred, and may be expected to
clear the condition in about 2–3 weeks, depending on the dosage used.
Treatment ladder
Localized disease,
recent onset
·
Topical terbinafine twice daily for
2 weeks
Or
·
Topical azole once or twice daily
for 2–4 weeks
Widespread disease
·
Oral terbinafine 250 mg/day 2–3
weeks
Or
·
Itraconazole 100 mg/day 2–4 weeks
Tinea capitis
Definition
This is ringworm of the scalp in
which there is invasion of the hair shafts by a dermatophyte fungus.
Age
It is generally a
disease of prepubertal children, especially those between the ages of 3 and 7
years, although adult cases are seen,
particularly with T. tonsurans infections.
Predisposing
factors
Predisposing factors for tinea capitis
include large family size, crowded living conditions, and low socioeconomic
class. In addition to transmission from other humans or animals, dermatophyte
spread via fomites (hairbrushes, combs, hats, and contaminated grooming
instruments).
Asymptomatic scalp
carriage of dermatophytes constitutes a major source of infection for
classmates and siblings. Asymptomatic carriage is most common with the
anthropophilic organisms T. tonsurans and T. violaceum. Household
contacts may be a significant source of asymptomatic carriers, and co-sleeping
and comb sharing seem to be important factors in the spread of disease in this
setting.
If actual hair infection is to
occur, invasion of the stratum corneum of the scalp skin must first develop.
Trauma assists inoculation, which is followed, after approximately 3 weeks, by
clinical evidence of hair shaft infection.
Causative
organisms
The causative
pathogens are members of only two genera: Trichophyton and Microsporum.
T. tonsurans is currently the most common cause of tinea capitis
(accounting for ≥90% of cases), and M. canis is the second most frequent
etiology.
Pathogenesis
Dermatophytes that invade hair shaft can occur in one of
three patterns and is dependent upon the species of dermatophyte involved:
ectothrix, endothrix and favus. Dermatophytes establish infection in the
perifollicular stratum corneum, entering the hair follicle orifice and then the
hair shaft. The funal organism penetrates only those hairs that are growing and
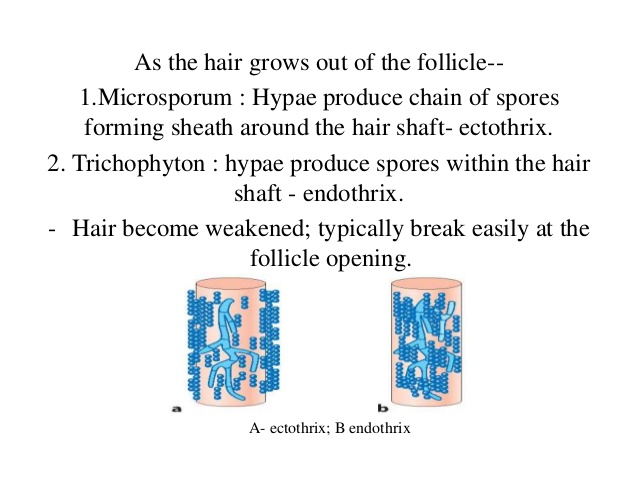
therefore affects anagen but not telogen hairs. As the hair grows outwards
hyphae are carried to the surface with production of arthroconidia. As a
consequence conida have been found in the air in close proximity to hair.
While in favus the infected hair
commonly grows to normal lengths, in endothrix infections where arthroconidia
are formed the hair shaft, being severely weakened, and breaks at the skin
surface. In small‐spored
ectothrix infections the shaft tends to fracture a few millimeters above the
surface.

Ectothrix type
Ectothrix
infections occur when both the inside and the outside of the hair shaft are
invaded and only the arthroconidia on the surface of the hair shaft may be
visualized, although hyphae are also present within the hair shaft. The intrapilary hyphae continue to grow inwards towards the
bulb of the hair, until the zone of incomplete keratinization is reached.
Growth is then arrested. Further up the shaft, hyphae from the existing
mycelium grow outwards from inside the hair and proliferate on its surface.
These secondary, extrapilary hyphae grow in a tortuous manner over the surface
of the hair shaft, which is growing outwards continuously. Small arthroconidia (2–3 μm diameters) are formed from
these fragmented secondary extrapilary hyphae outside the
hair shaft, which rapidly round up to become
spherical structures, and are seen as a packed mosaic of spores coating the
surface of the hair. This is the small‐spored ectothrix type of hair invasion and is clinically very
obvious and occurs as a dry scaling patch of alopecia with little inflammation
(that may mimic alopecia areata). This type of ectothrix infection is caused by
M. canis, M. audouinii and M.
ferrugineum. The cuticle of the hair is destroyed. On
Wood's lamp examination, a yellow–green fluorescence may be detected.
Other species of dermatophytes such
as T. verrucosum and T. mentagrophytes show different patterns of
hair invasion. Like the Microsporum species, they produce arthroconidia
on the surface of the hair and hyphae within it, but these conidia are larger
and are arranged in straight chains. This is known as large‐spored ectothrix hair invasion and clinically they present as boggy
inflammatory swelling known as a kerion.
Endothrix type
In endothrix infections only the inside of the hair shaft
is invaded and arthroconidia and hyphae remain within the hair shaft and leave
the cortex and cuticle intact. Intrapilary
hyphae fragment into arthroconidia up to 8 μm in diameter, which are entirely
contained within and completely fill the hair shaft. Hair thus affected is
especially fragile, and breaks off close to the scalp surface. Endothrix
organisms do not show fluorescence on Woods lamp exam. This pattern of tinea
capitis is associated with the appearance of “black dots” which represent
broken hairs at the surface of the scalp.
All endothrix-producing agents are anthropophilic (eg, Trichophyton tonsurans, Trichophyton
violaceum and Trichophyton
sudanense).
Favus
Favus is the most severe
form of dermatophyte hair infection and is most frequently caused by T.
schoenleinii. In favus, longitudinally arranged broad, regularly septate hyphae and air spaces are observed within the
hair shaft. Arthroconidia are not usually noted in infected hairs. The affected hair is less damaged than in other types, and
may continue to grow to considerable lengths. Blue-white fluorescence by Wood’s light
examination is typically seen. Favus presents as thick, yellow crusts composed
of hyphae and skin debris (“scutula”). Scarring alopecia may develop in chronic
infections.


Clinical
features
Tinea capitis predominates in healthy preadolescent
children (6 to 10 years of age); infants are less frequently affected. The
incidence in adults is generally low, but it is more commonly seen in the
immune compromised, where the presentation may be atypical.
The clinical appearance of tinea capitis is highly
variable, depending on the causative organism, type of hair invasion and degree
of host inflammatory response. Common features are patchy hair loss with
varying degrees of scaling and erythema. A number of clinical patterns
exist.
Clinical variants
Non inflammatory
Grey patch
Small-spored, ectothrix Microsporum infection typically
produces characteristic fine scaling with sharply
marginated circular patches of partial alopecia, but showing numerous broken‐off
hairs, dull grey from their coating of arthroconidia. Arthroconidia may
form a sheath around affected hairs turning them gray. Hair shaft becomes
brittle causing them to break off just above the level of the scalp giving the
appearance of mowed wheat field on the scalp. Small patches coalesce, forming
larger patches. Inflammation may be minimal with anthropophilic fungi (e.g. M.
audouinii, M. ferrugineum); however, zoophilic or geophilic species (e.g. M.
canis, M. gypseum) typically demonstrate more intense inflammatory response.
Endothrix
infections (black dots)
In T.
tonsurans and T. violaceum infections, a relatively non‐inflammatory patches of alopecia
with fine scale. Hairs broken off at the level of the scalp
surface leave behind grouped black dots (swollen hair shafts visible in the
follicular orifice) within patches of alopecia. Normal hairs also remain within
patches of broken hairs. The patches are usually multiple.
They are commonly angular in outline rather than round and tend to diffuse and
poorly circumscribed. While “black dot” tinea capitis tends to be minimally
inflammatory, some patients may develop follicular pustules, furuncle-like
nodules, or in rare cases kerion—a boggy, inflammatory mass studded with broken
hairs and follicular orifices oozing with pus.
Diffuse scale
In some cases, alopecia is minimal or absent and
infection presents as generalized, diffuse scaling of the scalp, resembling
dandruff.
Inflammatory
Diffuse pustular
In more inflammatory variants, a diffuse, patchy alopecia
may coexist with scattered follicular pustules. This may be associated with
painful regional lymphadenopathy.
Kerion
This is the term given to tinea capitis presenting as a painful
inflammatory mass with associated alopecia. It is characterized by boggy, purulent,
inflamed nodules and plaques. Hairs do not break off but full out and can be
pulled without pain. Follicles may discharge pus. A single plaque is usual, but
multiple lesions may occur with involvement of the entire scalp. There is
massive purulent secretion from multiple openings, (like the honey from a honey
comb). There may be sinus formation, and
on rare occasions mycetoma‐like grains may be found.
Thick crusting with matting of adjacent hairs is common. Regional
lymphadenopathy is common. This variant represents a delayed host inflammatory
response to the causative dermatophyte. Some patients may even become
systemically ill with fever and headache.
The lesions heal with scarring alopecia. Misdiagnosis
as bacterial abscess is common; however, secondary bacterial infection may
occur. Kerion is commonly seen with zoophilic, large-spore ectothrix species
(e.g. T. Mentagrophytes, T. verrucosum); however, this has been superseded in
recent years by endothrix infections with either T. tonsurans or T. violaceum,
particularly in urban areas.
Favus
A chronic, inflammatory tinea capitis typically seen in
T. schoenleinii infection, this variant is most commonly encountered in the
Middle East and North Africa. Early cases show perifollicular erythema and
matting of hair. Later, thick yellow adherent crusted, cup-shaped lesions
(‘scutula’) composed of hyphae and keratin debris that are pierced by remaining
hair shafts. The lesions produce a fetid odor and shows little tmdency to dear
spontaneously. Often results in scarring alopecia. Favus infections fluoresce
under Wood’s lamp.
Clinical diagnostic aids
Wood’s lamp
Ectothrix Microsporum species demonstrate bright green
fluorescence of infected hairs under Wood’s lamp examination. This may aid
clinical distinction from nonfluorescent Trichophyton infection (exception: T.
schoenleinii can fluoresce dull green).
Clinical
pearls
The presence of regional lymphadenopathy in combination
with alopecia and/or scale in a child suspected of having tinea capitis is an
important diagnostic clue and should encourage appropriate investigation with
fungal culture.
Histopathology
In tinea capitis, PAS and methenamine silver stains
readily reveal hyphae around and within hair shafts. The dermis demonstrates a
perifollicular mixed cell infiltrate with lymphocytes, histiocytes, plasma
cells, and eosinophils. Follicular disruption leads to an adjacent foreign-body
giant cell reaction. Markedly inflammatory lesions such as a kerion demonstrate
an acute infiltrate of polymorphonuclear leukocytes within the dermis and
follicle. Organisms may not be visualized in kerion since the intense host
response destroys many of the fungal organisms. However, fungal antigens may be
detectable with immunofluorescent techniques.
Differential diagnosis
The differential diagnosis of tinea capitis is extensive,
encompassing any condition causing patchy hair loss, scaling or scalp
inflammation. Scalp psoriasis, seborrheic dermatitis and atopic dermatitis may
be difficult to differentiate from noninflammatory tinea capitis, although
these conditions are usually more diffuse, and there may be characteristic
signs elsewhere. Alopecia areata is generally non scaly but may occasionally
demonstrate erythema. Exclamation-mark hairs must be distinguished from the
broken hairs of tinea capitis. Lupus erythematosus, lichen plano pilaris and
trichotillomania should also be considered, although they are relatively rare.
Inflammatory tinea capitis variants may be misdiagnosed as bacterial
folliculitis, folliculitis decalvans or abscesses. Regional lymphadenopathy may
be associated with inflammatory variants of tinea capitis.
Disease
course and prognosis
Without medication there is
spontaneous clearing at about the age of
15 years, except with T. tonsurans,
which often persists into adult life.
Treatment
Tinea
capitis requires oral therapy, because the drug needs to penetrate the hair
follicle. Both itraconazole and terbinafine
are now licensed for use in children. Terbinafine oral granules are now approved by
the FDA for treatment of tinea capitis in children 4 years of age and older. The best length of treatment for T. tonsurans and T.
violaceum infections with terbinafine appears to be 1 month. There is some
evidence that higher doses of terbinafine may be more effective for Microsporum.
Also
important in the management of tinea capitis are preventive measures. Because
the disease is contagious, all individuals residing with the infected patient
should be examined for signs of tinea capitis and appropriately treated.
Chronicity may develop if a child is continually re-exposed from untreated
family members. Concomitant therapy with an antifungal shampoo such as 2% ketoconazole
two to three times weekly is desirable for the patient because these agents may
aid in removing scales and eradicating viable spores, which may help decrease
the potential spread of infection and also for household contacts, until the
patient is free of disease. Also, combs, brushes and headwear used by the
patient should be disinfected or preferably discarded.
Topical
treatment alone is not recommended for the management of tinea capitis. Local
treatment with a topical antifungal with a fungicidal mechanism of action, such
as ciclopiroxolamine or terbinafine cream, may reduce the risk of infecting
other people and shortens the duration of systemic treatment. The entire hair
of the scalp in all its length should be treated with the antifungal. Treatment
should be administered once daily for approximately 1 week.
The
treatment of kerion deserves special mention. These markedly inflammatory
reactions may result in permanent scarring alopecia, and therefore rapid
institution of aggressive therapy is indicated. In addition to antifungal
therapy, careful removal of crusts using wet
compresses
and systemic antibiotics should be considered, especially in the presence of
significant crusting, because secondary bacterial infection may concomitantly
occur. Skin swab for bacterial culture and sensitivity may be useful in this
setting to guide the choice of antimicrobial. Oral glucocorticoids may reduce
the incidence of scarring associated with kerions. Although there is no
consistent evidence for improved cure rates with use of oral glucocorticoids,
they appear to relieve pain and swelling associated with infections. The usual
regimen prednisone is 0.5 to 1 mg/kg
per day each morning during the first week of antifungal therapy.
Treatment ladder
· Terbinafine: <10 kg, 62.5 mg; 10–20 kg, 125 mg; >20
kg, 250 mg. All given daily for 4 weeks
· Itraconazole 2–4 mg/kg/day for 4–6 weeks
Itraconazole
capsule: simplified dosing:
10-20 kg: 100 mg every other day
21-40 kg: 100 mg daily
>40 kg: 200 mg daily
Tinea barbae
Definition
This is ringworm of the beard of the
face and neck including moustache area with the invasion of terminal hairs. It
is thus a disease of the adult male. Tinea of the chin and upper lip in females
and children are considered to be tinea faciei (ringworm of the glabrous skin
of the face).
Predisposing
factors
Disease is
often acquired from animals. In the past, a common cause of infection was
contaminated razors in barbershops. With the increased use of disposable razors
and disinfectants, however, the incidence of tinea due to this source has been
dramatically reduced.
Pathology
Infections
with T. mentagrophytes and T. verrucosum lead to large‐spored ectothrix invasion with the
spores in chains. The other less commonly involved species produces their own
characteristic types of hair invasion.
Causative
organisms
The causative organisms are typically
zoophilic dermatophytes, namely T. mentagrophytes and T. verrucosum.
Clinical
features
Tinea barbae affects the face unilaterally and involves
the beard area more often than the moustache. Two forms exist.
Inflammatory Type
The affected men are commonly farm workers. Since zoophilic organisms are the most common culprit and
affected areas often have a large number of terminal hair follicles, the
clinical presentation tends to be severe, with intense inflammation and
multiple follicular pustules. Follicular pustules may coalesce and
eventuate in abscess-like collections of pus, sinus tracts, bacterial super
infection, kerion-like boggy- crusted plaques and scarring alopecia. Hairs
within the affected areas are lusterless, brittle and loose and easily removed
with the forceps without causing pain to demonstrate a purulent mass around the
root. Patients may have constitutional symptoms such as malaise as well as
lymphadenopathy. After 4-6 weeks, these inflammatory lesions settle
spontaneously with a degree of immunity, as second bouts are unlikely.
Superficial Type
Caused by anthropophiles such as T.
rubrum, this form of tinea barbae is superficial,
less inflammatory and resembles tinea corporis or bacterial
folliculitis. Consist of dry, circular, reddish, scaly patches. Alopecia may be
present in the centre of the lesion in which hair is broken off at the surface but
it is reversible. Scattered follicular papules, pustules and small nodules that
may be easily mistaken for Staphylococcus aureus folliculitis may develop.
Differential
diagnosis
The
classic, highly inflammatory lesions are distinguished from boils by their
relative lack of pain. Loosened hairs, although present in some bacterial
infections, are rarely as obvious as they are in tinea barbae. The presence of Staphylococcus
aureus on a swab taken from lesions in this area does not exclude ringworm,
as bacterial colonization or frank co‐infection may occur in tinea barbae. Unfortunately,
mycological cultures are often negative.
Treatment
Beard infections usually respond satisfactorily
to itraconazole or terbinafine, sometimes in combination with topical therapy
over a period of 4–6 weeks. Fairly long‐term follow‐up
is recommended, and late recurrences undoubtedly occur.
Tinea
faciei
Definition
Tinea faciei is infection of the
glabrous skin of the face with a dermatophyte fungus (the moustache and beard
areas of the adult male are excluded).
Predisposing
factors
Facial
skin may be infected either by direct inoculation of a dermatophyte fungus from
an animal (e.g. T. mentagrophytes from an infected pet) or there may be
secondary spread from pre‐existing
tinea of another body site. The latter pattern is likely to occur with T.
rubrum as well as with T. concentricum infections.
Clinical
features
Tinea infection of the face is
frequently misdiagnosed. Typical annular rings are usually lacking and the
lesions are highly photosensitive. Erythema
is usual, but scaling is present in less than two‐thirds of cases. A substantial proportion of patients do
show annular or circinate lesions, and induration with a raised margin is
present in about half. Simple papular lesions, and in some cases completely
flat patches of erythema, also occur. A few vesicles or pustules may be found,
but these are rarely conspicuous. The application of topical steroids may further
modify the appearance.
Differential
diagnosis
Because
of light sensitivity, the frequent absence of scaling and the somewhat
nondescript appearance, this condition may be confused with discoid lupus
erythematosus (DLE) and polymorphic light eruption. Moreover, tinea faciei
coexisting with DLE has been described. Reluctance to biopsy the face adds to
the problem, but if there is possibility of tinea faciei, careful examination
and scrapings taken from the skin surface, even if this is not obviously scaly,
should enable a diagnosis to be made. If topical steroids have been applied, a
cessation of the therapy may be followed a few days later by a great increase
in scaling and by appearances much more readily diagnosable.
Treatment
In localized cases, if promptly
diagnosed, topical therapy seems to work well, especially with one of the
imidazoles. Where delay has occurred before the diagnosis is established, and
especially when steroid therapy has modified the condition, terbinafine or
itraconazole is generally preferred. Most cases will clear in 3 or 4 weeks,
certainly in 6 weeks, but longstanding infections may occasionally need longer
periods of treatment.
Tinea pedis
Definition
Tinea
pedis is a dermatophyte infection of the soles and interdigital web spaces of
the feet. Infection of the dorsal aspect of the foot is considered tinea
corporis. The term athlete's foot is used to
imply any form of toe cleft intertrigo. In this context, the terms tinea pedis
or foot ringworm is preferred, which clearly exclude infections caused by
bacteria, Candida and non‐dermatophyte moulds. The feet are the most common location for
dermatophyte infections.
Age
The
condition is more common in adults than children.
Sex
Adult
males more commonly develop tinea pedis than women.
Predisposing
factors
The lack of sebaceous glands and the moist
environment created by occlusive shoes are important factors in the development
of tinea pedis, which is in most cases initially a
lateral web space infection. In fact, tinea pedis is uncommon in populations that do
not wear shoes. However, the fungus may be acquired from going barefoot (locker
rooms, gyms, public facilities).
The spores of dermatophytes survive for months in shoes,
carpets, bath mats and showers. The warm moist microenvironment in shoes,
coupled with reduced hygiene, hyperhidrosis, increasing age and poor peripheral
blood flow are predisposing factors. Using rubber sandals in showers, carefully
drying the feet, especially between the toes, and wearing clean shoes and socks
are possible preventive measures.
Pathology
The
moist conditions of the toe clefts cause maceration and damage the stratum
corneum at the same time that probably favors growth of the fungus. A
simultaneous increase in the resident bacteria flora, such as large‐colony coryneforms, may be acting as
important co‐pathogens.
Causative
organisms
The
dermatophytes that are typically responsible for tinea pedis are T. rubrum, T. interdigitale (previously T. mentagrophytes var. interdigitale), T. mentagrophytes, E. floccosum, and T. tonsurans (in
children). Non-dermatophyte pathogens that produce clinical findings identical
with tinea pedis include Neoscytalidium dimidiatum and N. hyalinum (moccasin and interdigital types) and,
occasionally, Candida spp. (interdigital
type).
To some extent, fungal species correlates with the clinical forms.
Clinical
features
Tinea pedis may present as any of four forms, or
combinations thereof.
Interdigital Type
This common type is predominantly
affecting the interdigital and subdigital skin of the feet, and in particular the
lateral two toe clefts because they are the tightest of the interdigital spaces
and caused by any of the three species. When one spreads the
toes, one may find gray-white swollen macerated skin. When the macerated skin
is removed, peeling, erosions, fissures, and erythema may be prominent. Under
appropriate conditions, the infection will spread to the adjacent sole or
instep, but it rarely involves the dorsum. Two aggravating factors are
hyperhydrosis and gram negative bacterial coinfection such as pseudomonas and
proteus that soon produce the malodor that are characteristic of the
dermatophytosis complex (fungal infection followed by bacterial invasion), or
“athlete's foot.”
Chronic Hyperkeratotic
(Moccasin) Type
In
T. rubrum infections, a chronic hyperkeratotic type of tinea pedis is seen. There is patchy or diffuse hyperkeratosis,
erythema, fine silvery white scales and fissures on one or both the soles,
heels and the lateral and medial aspects of the feet, in a distribution similar
to a moccasin on a foot. The arciform pattern of scales is characteristic. On
careful examination, as the scales proceeds along the edge of the foot,
erythema at the advancing border may be seen. There may also exist few minute
vesicles that heal with collarets of scale less than 2 mm in diameter. The
dorsal surfaces of the toes and feet are not often affected, but associated
nail infection is very common.
Frequently chronic and difficult to
cure because of the thickness of stratum corneum on planter surface and the inability of T. rubrum to elicit an
immune response sufficient to eliminate the fungus.
Vesiculobullous Type
Vesiculobullous type of tinea pedis,
typically caused by zoophilic strains of T. interdigitale. Sudden eruption of
pruritic grouped vesicles, usually on the instep. The vesicles may become
pustules and may coalesce forming large bullae that eventually shed their
roofs, producing characteristic erosions with scale and erythema at the edge.
The roof of such a blister is an ideal specimen for KOH examination. This variety of ringworm frequently goes on to apparent
spontaneous cure, but tends to recur in warm weather.
Acute Ulcerative Type
Typically an exacerbation of interdigital tinea pedis,
secondarily infected with Gram-negative bacteria produces pustules and purulent
ulcers in the web spaces; seen in immunocompromised and diabetic patients.
Vesiculobullous and acute ulcerative types commonly
produce a vesicular Id reaction, either on the lateral foot or toes, or on the
lateral aspects of the fingers.
Complications
and co‐morbidities
Each type has different
associated morbidities and complications that can affect diagnostic considerations
and therapeutic options. These include bacterial superinfection (the
“dermatophytosis complex”), dermatophytid reactions, cellulitis (especially in
patients who have venous hypertension, harvested saphenous veins, and chronic
edema), and even osteomyelitis leading to amputation in diabetics. Oral antifungal therapy should be considered
in diabetics, immunocompromised patients, and those with moccasin-type tinea
pedis. Finally, other dermatophyte infections often occur together with tinea
pedis – in particular, tinea cruris, onychomycosis, and tinea manuum – and
these sites should be examined.
Treatment ladder
Mild
and moderate interdigital disease
·
Topical imidazole twice daily for 4
weeks
·
Topical terbinafine twice daily for
7 days
·
Tolnaftate powder
Dry
type tinea pedis
·
Terbinafine 250 mg/day for 2 weeks
Or
·
Itraconazole 400 mg/day for 1–2
weeks
Tinea manuum
Definition
Dermatophyte
infections on the dorsal aspect of the hand have a clinical presentation
similar to tinea corporis. However, dermatophyte infection of the palm and
interdigital spaces has distinct characteristics with infections beginning
under rings and is referred to as tinea manuum. The reason for the two
different clinical pictures is thought to be related to the lack of sebaceous
glands on the palms.
Predisposing
factors
In
most cases there is pre‐existing
foot infection with or without toenail involvement. A special mention should be
made of ringworm beginning under rings and wrist watches, and occupational
usage predispose to maceration between the fingers. Poor peripheral circulation
and palmar keratoderma are other possible predisposing factors.
Causative
organisms
The typical
causative organisms are the same three anthropophilic species involved in tinea
pedis and tinea cruris: T. rubrum, T. mentagrophytes and E.
floccosum. Two non-dermatophyte fungi that cause “tinea manuum” are Scytalidium
dimidiatum and S. hyalinum.
Clinical
features
Tinea manus is almost always secondary to tinea pedis as
infection of the hand is acquired from excoriating and picking infected feet
and toenails.
Most commonly only one hand (singular: tinea manus) is
involved, concomitant with infection of both feet (Mosaic-type) and toenails
for which the term “two feet–one hand” syndrome has been coined and the two
share clinical features such as chronicity and hyperkeratosis. The hand
affected is often the dominant one, suggesting that direct inoculation onto the
more active hand is likely. Trichophyton
rubrum infection may
take several different clinical forms.
The most common variant is the hyperkeratotic form, there
is diffuse fine, firmly adherent, dry scaling on an erythematous background of
the palms and fingers, often accentuated in the flexural creases, that fails to
respond to emollients. The hands feel very dry and rough. However,
circumscribed vesicular and pustular patches may be present, especially when
zoophilic dermatophytes involved. Tinea unguium of
the involved hand can serve as a clue to the diagnosis, but infection of all
the fingernails is uncommon.
Differential
diagnosis
Dermatophyte
infections of the palm are often quiet and chronic, commonly passing unnoticed
or misdiagnosed. One must always check the
feet and groin. If the changes are symmetric, psoriasis or dermatitis is more
likely, while asymmetric or unilateral changes suggest tinea. When the
interdigital spaces or nail folds are involved, candidiasis is strongly
indicated.
Unilateral
scaling should always alert the clinician to the necessity of taking scrapings.
Nail changes may help: pitting suggests psoriasis, but subungual hyperkeratosis
if present should always be scraped. If the palmar infection spreads to the
dorsal surface, more classic annular lesions may be seen, although this happens
relatively infrequently. Tinea manuum, like tinea cruris and tinea faciei, is
sometimes modified by inappropriate treatment with topical steroids leading to
further diagnostic difficulties.
Treatment of tinea
Pedis and Manuum
Mild
and moderate interdigital
tinea pedis without bacterial involvement is treated topically with allylamine,
imidazole, ciclopirox creams. Topical imidazole is applied twice daily for 4 weeks. Terbinafine cream applied twice
daily for 1 week is effective in 66% of cases. For dry type tinea pedis oral antifungal is required. The dosing schedule
of oral terbinafine is 250 mg daily for 2 weeks. Itraconazole in adults is given
400 mg daily for 1 week, 200 mg daily for 2–4 weeks, or 100 mg daily for 4
weeks with similar efficacies of all regimens, whereas itraconazole in children
is administered at 5 mg/kg/day for 2 weeks. Fluconazole 150 mg weekly for
3–4 weeks is also effective. Topical or systemic corticosteroids may be helpful
for symptomatic relief during the initial period of antifungal treatment of
vesiculobullous tinea pedis. Maceration, denudation, pruritus, and malodor
obligate a search for bacterial coinfection by Gram stain and culture, the
results of which most often demonstrate the presence of Gram-negative organisms
including Pseudomonas and Proteus. Patients suspected of having Gram-negative
coinfections should be treated with a topical (potassium permanganate followed by a topical antifungal is preferred)
or
systemic antibacterial agent based on the culture and sensitivity report.
Associated onychomycosis is common; if present, more durable treatment of the
onychomycosis is necessary to prevent recurrence of tinea pedis.
Chronic ringworm infections of the
palm are not easily cleared, and oral therapy is always needed. Itraconazole
and terbinafine are both effective in this condition. Most cases clear with 2–4
weeks of treatment.
Tinea cruris
Definition
Tinea
cruris is a dermatophyte infection of the inguinal region, in particular the
inner aspects of the upper thighs and crural folds, with
occasional extension onto the abdomen and buttocks. It is the second-most common type of
dermatophytosis worldwide.
Epidemiology
This disease is more
often seen in adult men than in women, since the scrotum provides a warm and
moist environment that encourages fungal growth and men are more likely to have
tinea pedisand onychomycosis as a source of
dermatophytes.
Predisposing
factors
Tinea cruris is frequently associated
with tinea pedis because clothing that is brought over the feet is contaminated
and then comes in contact with skin in the groin region. The old advise>
Always put your socks on before your underwear. Thus, one should check the feet
of all patients with groin rashes. Finally, all the factors that lead to
intertrigo, such as obesity, inadequate personal hygiene, hyperhydrosis,
prolonged sitting on plastic or non-absorbent surfaces, tight synthetic
clothing, and even diabetis mellitus, may play a role. It is common during the hot summer when the humidity is high.
Causative
organisms
T.
rubrum is the main cause; T.
interdigitale and E. floccosum also account for some cases.
|
TINEA CRURIS: COMMON CAUSATIVE PATHOGENS |
|
|
Dermatophyte |
Clinical features |
|
Trichophyton rubrum |
1.
Most common cause of tinea cruris 2.
Infection tends to be chronic 3.
Fungus not viable in scale (e.g. on furniture, rugs,
linens) for long periods of time 4.
Frequent extension of infection from the groins to the perianal,
buttocks, the lower back, pubic and lower abdomen is common. The penis is
occasionally affected. |
|
Epidermophyton floccosum |
1.
Commonly associated with “epidemics” of tinea cruris in
locker rooms or dormitories 2.
Infection is acute (rarely chronic) 3.
Arthroconidia are viable in scale (e.g. on furniture,
rugs, linens) for long periods of time 4.
Infection limited to the genitocrural crease and the
medial upper thigh 5.
Causative agent of “eczema marginatum” (well-demarcated
borders with multiple small vesicles or, sometimes, vesiculopustules) |
|
T. mentagrophytes,
in particular var. mentagrophytes |
1.
Infection tends to be more severe and acute, with
intense inflammation and pustule formation 2.
May rapidly spread to the trunk and lower extremities,
causing a severe inflammatory condition 3.
Often acquired from animal dander |
Clinical
features
The initial sign of
infection is usually an area of erythema and pruritus in the fold between the
scrotum and the inner thigh. Characteristic lesions are well demarcated annular erythematous
plaques, curved with sharp margins with a scaly raised advancing border that
may contain pustules or even vesicles extending from the groin fold down the
upper inner aspect of the thighs, just where the scrotum usually touches the
leg. Dermal nodules forming beading along the edge are commonly found in older
lesions. Pruritus is common, as is pain when plaques are macerated or
secondarily infected. The disease can remain unilateral or become bilateral.
The duration of infection depends on
the causative pathogen. Infections with T. rubrum tend
to be chronic, sometimes with leathery and lichenified lesions. In contrast,
the zoophilic form of T. mentagrophytes (previously T. mentagrophytes var. mentagrophytes) often causes acute infections with a
prominent inflammatory component that may include pustules. The scrotum itself
is generally spared in tinea cruris. If the scrotum is involved or there are
erosions or satellite pustules, cutaneous candidiasis should be considered.
Differential
diagnosis
Candidosis, which is more common in
women, does not have a distinct raised margin. White pustules are often found,
satellite lesions are numerous and small, and often produces collarette scale as the tiny pustules rupture is characteristic. Pityriasis
versicolor may be localized to the groin but is usually non‐inflammatory and asymptomatic, as is
erythrasma. Central clearing is rarely found in either of these infections.
Treatment
In cases of recent onset, topical
therapy can be expected to be curative within 2–4 weeks. Topical terbinafine
and the imidazoles are better tolerated in the flexural areas, and if the
diagnosis is in doubt terbinafine and the imidazoles have the advantage of
being effective against Candida as well. Where the condition has been
present for many months, or has spread to the pubic area, the natal cleft or
the buttocks, and where topical steroids have been used, systemic treatment is
strongly recommended. Oral terbinafine and itraconazole usually produce a
remission in 1–2 weeks. Some patients relapse even after this therapy and a
longer course of therapy may work in these recalcitrant cases.
Treatment ladder
Recent‐onset disease
·
Topical terbinafine or imidazoles
twice daily for 2 weeks
Chronic
or extensive disease
·
Oral terbinafine 250 mg/day for 1–2
weeks
Or
·
Itraconazole 100 mg/day for 2–4
weeks
Infection control
The reduction of perspiration and
enhancement of evaporation from the crural area are important prophylactic
measures. The area should be kept as dry as possible, especially drying thoroughly
after bathing, wearing of loose underclothing and trousers, plain talcum powder
or antifungal powders are helpful, weight reduction (if obese), laundering
contaminated clothing and linens, and treating concomitant tinea pedis. Greater
control of tinea pedis might lead to fewer cases of tinea cruris. A person
suffering from tinea pedis or cruris should not lend towels to others, even if
they have been laundered.
Onychomycosis
Definition
Onychomycosis is a fungal
infection of the toenails or fingernails that may involve any component of the
nail unit, including the matrix, bed, or plate. The infection may be due to a dermatophyte, yeast, or
non dermatophyte mould. The term "tinea unguium" is used specifically
to describe invasive dermatophytic onychomycosis.
The disease course is chronic.
Epidemiology
The disease is twice
more frequent among men than women, and it seems to increase with age.
Onychomycosis is the
most prevalent nail disease and accounts for approximately 50% of all causes of
onychodystrophy. It affects up to 14% of the population with an increasing
prevalence among older individuals. Onychomycosis is also increasing in incidence
among children and adolescents and accounts for up to 20% of dermatophyte
infections diagnosed in children. Risk factors for nail infection include nail
trauma, immunosuppression such as HIV infection, diabetes mellitus, and
peripheral vascular insufficiency. The increasing prevalence of this disease
may be secondary to wearing of tight shoes, increasing numbers of individuals
on immunosuppressive drugs, and an increased use of communal locker rooms. The
dermatophytosis commonly begins as tinea pedis before extending to the nail
bed, where eradication is more difficult. This site serves as a reservoir for
local recurrence or for infections spreading to other areas. Up to 40% of
patients with toenail onychomycosis show concomitant skin infections, most commonly
tinea pedis (30%).
Causative
organisms
A variety of fungi have been
implicated in the causation of OM. Most commonly, the source of infection is
the infected surrounding skin and the same organism is detectable from both
sites. Dermatophytes account for ~90% of cases of onychomycosis, and the
remainder are due to yeasts or non-dermatophyte molds. Although
all dermatophytes can cause tinea unguium, Microsporum spp.
does so very rarely. The most common causative pathogens are T. rubrum, T. interdigitale, T. tonsurans (in
children), and E. floccosum. Yeasts generally invade already
damaged nails (like in chronic paronychia) or nails in immunosuppressed (as in
chronic mucocutaneous candidiasis). Candida albicans is the
most common yeast responsible followed by C. parapsilosis. Among
NDM, the commonly isolated species are Aspergillus and Scopulariopsis
brevicaulis. Although, there is still much debate as to whether
most NDMs actually cause nail infection or they are mere laboratory
contaminants or secondary invaders of already damaged nails, the accumulating
evidence highly suggests that some NDMs can be true primary invaders.
Although
nail infections may be the only manifestation of fungus disease in a patient,
in the great majority of cases they are associated with tinea pedis or tinea
manuum. Toenail infections are considerably more common than fingernail
infections, and only rarely does fingernail onychomycosis occur without
concurrent toenail infection. A single nail may be involved, but more commonly,
multiple nails on one or both hands or feet are affected.
Interestingly, about 50% of cases of
fingernail-related onychomycosis are caused by Candida spp, whereas
non dermatophyte molds are not detected in diseased fingernails. Onychomycosis
due to dermatophytes occurs more frequently in toenails than in fingernails.
Conversely, candidal onychomycosis more commonly affects the fingernails. In
addition, most episodes of Candida onychomycosis begin as paronychial
infections ("whitlow"). In other words, infection begins in the
structures around the nail rather than in the nail itself. Again, the opposite
is generally true of dermatophytic onychomycosis.
|
NON-DERMATOPHYTE
MOLDS THAT CAN CAUSE ONYCHOMYCOSIS |
|
|
Fungus |
Key features |
|
Fusarium spp. |
Superficial white
pattern* |
|
Aspergillus spp. |
Superficial white
pattern* |
|
Acremonium |
Superficial white
pattern* |
|
Scopulariopsis brevicaulis |
Lateral yellow–brown
discoloration |
|
Neoscytalidium hyalinum |
Distal and lateral
nail invasion† |
|
Neoscytalidium dimidiatum |
Distal and lateral
nail invasion† |
* Deeper
invasion of the nail plate can also occur.
† May also
be associated with paronychia or tinea pedis.
Both mechanical and chemical
factors have a role to play in the Invasion of nail apparatus by fungi. The
essential steps are surface adhesion followed by invasion into the sublayers.
The site and pattern of invasion which leads to production of different
clinical types of OM can be seen from [Figure]. Nail involvement occurs by penetration of
fungal elements and secretion of enzymes that degrade the skin components.
Dermatophytic fungi have been shown to have keratinolytic, proteolytic and
lipolytic activities. The hydrolysis of keratin by proteinases
not only facilitates invasion into tissues, but also provides nutrition to the
fungi. Nails being skin appendages undergo essentially the same pattern of
invasion. However, the nail apparatus has some unique features to offer.
The knowledge of the immune
mechanisms operative in the nail apparatus is still preliminary. Structurally,
the nail apparatus is exposed to a harsh environment and is prone to damage and
invasion by various organisms. The unique anatomy of the nail is prone to
provide easy portals of entry to pathogens, through the proximal nail fold and
the distal nail edge. However, these are physically protected by the cuticle
and the distal solehorn, respectively [Figure]a. The nail apparatus has
certain essential immunological differences as compared to that of skin. The
nail unit is isolated from the body's cell-mediated immunity (CMI). It is a site of relative immune privilege due to a very low
level of expression of MHC (Major histocompatibility) Class 1a antigens, local
production of potent immunosuppressive agents, dysfunction of antigen
presenting cells (APC) and inhibition of Natural Killer (NK) cell activity. Also,
dermatophytes are strongly keratinophilic organisms. This is because of their
ability to form perforating organs due to which they quickly digest
keratin. On the other hand, there are various protective mechanisms at
play as well. Nail unit has been shown to possess a strong innate
immunity. There is increased local expression of
antimicrobial peptide (human cathelicidin LL-37) in the nail. Cathelicidin
LL-37 is not expressed in human skin under normal circumstances, but it gets
induced upon exposure to infection or inflammation. However, it is strongly
expressed in the nail unit. Being a soluble antimicrobial, it has been shown to
have potent activity against Pseudomonas aeruginosa and Candida
albicans. In addition, a differential distribution of immune
cells has been observed in different parts of the nail apparatus. There is a
high density of CD4+ cells in the proximal nail fold (PNF) and very low density
in the proximal nail matrix (PNM). CD8+ T cells are rarely
seen in and around PNF, nail bed, and PNM. The density of Langerhans cells is
higher in epithelium of the PNF and nail bed as compared to that of the nail
matrix. The Langerhans cells and macrophages in the nail matrix are
functionally impaired with respect to their capability of antigen presentation.
In short, due to a lack of effective
cell-mediated immunity, the nail apparatus is susceptible to invasion by fungal
organisms, if it gets exposed due to various predisposing factors. Hence, OM is
usually a chronic infection not associated with inflammation. The nail plate
offers an ideal ecological niche for fungal organisms where they can persist
for long durations. Any physical compromise of the protective and
self-containing structure of the nail apparatus exposes it to an early invasion
by fungi which are then very difficult to eradicate.
Physical restrictions to the microbial invasion
of nail also get compromised under certain circumstances. Various predisposing
factors include vascular diseases, atopy, obesity, diabetes and sports.
Most patients with Candidal OM are involved in occupations that predispose to
repeated minor trauma or are engaged in domestic activities which involve wet
work. It is known that most dermatophyte species affect the ventral
and middle layers of the nail plate, where the keratin is comparatively soft,
and in close proximity to the underlying living cells. On the ventral surface,
the junctions between cells are more flexible than the tight junctions in the
dorsal part. The ventral surface has a highly irregular topography with
parallel grooves and ridges providing excellent channels for hyphae to
penetrate the nail plate. Also, the intercellular
junctions in the ventral plate are more flexible than the tight junctions in
the dorsal nail plate. The intermediate layer is involved less commonly, while
the dorsal nail plate is rarely involved except in case of white superficial
onychomycosis. The
dorsal nail plate is the hardest part and has increased calcium content.
Species differences in fungal pathogenecity have
also been reported with Trichophyton mentagrophytes being a more
active destroyer than Trichophyton rubrum. This active
pathogenecity for the nail could be a result of mechanical or enzymatic
processes.

Figure: Pathogenesis of Onychomycosis (a)
Anatomical structure of the normal nail unit. (b) Pattern of fungal invasion in
distal lateral subungual onychomycosis. (c) Pattern of fungal invasion in
endonyx onychomycosis. (d) Pattern of invasion in superficial white
onychomycosis. (e) Pattern of invasion in PSOM. (f) Fungal involvement in a
case of TDOM
Clinical
features
The pattern of
invasion, if correlated clinically, can be seen to give rise to different
clinical types of OM [Figure]b-f.
Onychomycosis has 5 main subtypes, as
follows:
·
Distal
lateral subungual onychomycosis (DLSO)
·
Endonyx
onychomycosis (EO)
·
White
superficial onychomycosis (WSO)
·
Proximal
subungual onychomycosis (PSO)
·
Candidal
onychomycosis
Patients may have a combination of these
subtypes. Total dystrophic onychomycosis, the most advanced form of any
subtype. Presentation varies by subtype.
Distal
lateral subungual onychomycosis (DLSOM): [Figure]b.
DLSO is the commonest clinical type of
onychomycosis. It begins with invasion of the stratum corneum of the
hyponychium. The infection then progresses to involve the nail bed and
subsequently the ventral nail plate. The infecting organism migrates proximally
through the nail plate (against the tide of growth of the nail plate). Hyperproliferation or altered differentiation of
the nail bed in response to the infection results in subungual hyperkeratosis.
With further progression of infection, there is yellowing, crumbling and
thickening of the distal nail plate as well as distal onycholysis, which
provides an ideal environment for further proximal invasion and growth of the
dermatophyte. Yellow streaks in the central portion
of the nail plate are commonly observed. Eventually, the entire nail bed
and plate may become involved (total dystrophic pattern).
Although commonly starting with a single affected nail,
other digits later become invaded. Toenails are involved much more commonly
than fingernails. First and fifth toenails are infected most frequently.
Involvement of the fingernails is usually unilateral. When fingernails are
involved, pattern is usually two feet and one hand.
This
type is usually caused by dermatophytes, especially T. rubrum and
less commonly T. mentagrophytes, T. tonsurans,
and E. floccosum.
Endonyx onychomycosis (EOM):[Figure]c.
In this variant,
there is a primary and exclusive attack on the nail plate with the fungus
growing between the nail plate lamellae. This pattern of invasion is specific
for T. soudanense (and possibly T. violaceum)
and may reflect its high affinity for hard keratins. Clinically,
EOM is seen as a diffuse milky-white discoloration of the affected nail plate, forming irregular wide waves with pits and lamellar splits, but,
in contrast to distal lateral subungual onychomycosis, no evidence of subungual
hyperkeratosis or onycholysis is present.
Nail plate surface and nail thickness are normal. A large number of fungal hyphae are visible within the
nail plate with absence of fungal elements in the nail bed and
hyponychium.
Superficial white onychomycosis (SWO)[Figure]d.
It is less common than DSO (estimated
proportion of onychomycosis cases, 10%) and occurs when fungi invade the dorsal part of the nail plate directly.
The dorsal surface of the nail plate is eroded in well-circumscribed powdery
white patches, often away from the free edge. The
nail becomes roughened and crumbles easily. It is distinguishable from
other causes of leukonychia by the powdery nature of the white material, which
can easily be scraped away, revealing a solid nail underneath. The white
patches then coalesce and spread to involve the whole surface of the nail
plate. SWO occurs primarily in the toenails. Molds
produce a deep variety of white superficial onychomycosis characterized by a
larger and deeper nail plate invasion.
The most common etiologic agent in SWO
is T. interdigitale, although non dermatophyte molds such as Aspergillus,
Scopulariopsis, and Fusarium are also known pathogens. Candida species may
invade the hyponychial epithelium to eventually affect the entire thickness of
the nail plate.
In HIV patients,
SWO has been documented in fingernails as well, and is generally caused
by T. rubrum and superficial infection may coexist with
proximal white subungal onychomycosis
Proximal white subungal onychomycosis
(PWSO):[Figure]e.
A
relatively uncommon subtype, and occurs when organism first invades stratum corneum
of the proximal nail fold and then penetrates to the nail matrix and the
undersurface of the newly formed nail plate, and migrate distally. Clinically, PWSOM presents as an area
of leukonychia in the proximal nail plate that moves distally with nail growth. Other
features are proximal onycholysis, subungual hyperkeratosis and destruction of
the proximal nail plate. It may also present as a pattern of proximal to distal
longitudinal leukonychia affecting a single digit, an isolated transverse
leukonychial band, or multiple transverse bands separated by areas of normal
nail. This pattern has been described in both finger and toenails.
In proximal subungual onychomycosis caused by molds, leukonychia
is typically associated with marked periungual inflammation.
T. rubrum is
the commonest causative agent. Patients with PSO should be screened for HIV, as PSO has
been considered a marker for this disease.
Candida onychomycosis
Nail invasion by Candida is not common
because the yeast needs an altered immune response as a predisposing factor to
be able to penetrate the nails. Despite the frequent isolation of Candida from the
proximal nail fold or the subungual space of patients with chronic paronychia or onycholysis, in these
patients Candida is
only a secondary colonizer. In chronic mucocutaneous
candidiasis,
the yeast infects the nail plate and eventually the proximal and lateral nail folds.
In patients with chronic mucocutaneous candidiasis or
immunodepression, several or all digits are affected by total onychomycosis
associated with periungual inflammation. The digits often take on a bulbous or
drumstick appearance.
Total dystrophic
onychomycosis (TDOM): [Figure]f
This type presents as total destruction of the entire nail apparatus including whole thickness of the plate, the nail bed and matrix. The involved nail becomes crumbles and disappears, leaving behind an abnormal thickened nail bed. It may be primary e.g. in cases with chronic mucocutaneous candidiasis or secondary to any of the four previous forms.

Laboratory Studies
OM has distinct
clinical presentation, however, the key features are shared with other
onychopathies like psoriasis and lichen planus. Hence, clinical examination in
isolation is seldom sufficient to make a diagnosis of OM. Therefore,
laboratory diagnosis of onychomycosis must be confirmed before beginning a
treatment regimen. A negative mycological result does not rule out
onychomycosis, because direct microscopy may be negative in up to 10% of cases
and culture in up to 30% of cases.
The
diagnosis of NDM OM is based on the presence of at least three of the following
six criteria. These include identification of NDM in nail by direct microscopy;
isolation of NDM in culture; repeated isolation in culture; inoculums counting;
failure to isolate a dermatophyte in culture; and histology.
|
|
|
|
|
|

Algorithm for the laboratory diagnosis of OM
Sampling techniques
Isolation of the fungal pathogen
from nail is reportedly more difficult than for skin and hair. Conventionally,
the material is taken from the distal end of the nail, despite the fact that
the infection is advancing proximally. The hyphae at the distal end of the nail
are less likely to be viable, hence less likely to grow on culture
media. Hence, culture results improve if samples are taken from more
proximal sites. Proximal sampling may be more uncomfortable for the patients
but it should be the norm as far as possible.
Nail clippers should be used to include full
thickness of the nail. Subungual debris is a good source with superficial
scrapings being helpful only in cases of SWO. Culture sensitivity from samples
collected by drilling techniques has been found to be statistically superior to those collected by curettage. Drilling technique can be
horizontal or vertical (especially useful for PSOM). In an
Indian study, the use of dental drill for collection of nail samples
significantly improved the culture yield for fungus.
Conventional methods of identifying causative
organisms
Direct microscopy
A 20% potassium hydroxide (KOH)
preparation in dimethyl sulfoxide (DMSO) is a useful screening test to rule out
the presence of fungi. Before obtaining a specimen, the nails must be clipped
and cleansed with an alcohol swab to remove bacteria and debris. The
preparation does not require heating or prolonged incubation if DMSO is a
component of the KOH solution.
In distal lateral subungual
onychomycosis, a specimen should be obtained from the nail bed by curettage.
The onycholytic nail plate should be removed and the sample should be obtained
at a site most proximal to the cuticle, where the concentration of hyphae is
greatest.
In proximal subungual
onychomycosis, the overlying nail plate must initially be pared with a No. 15
blade. Then, a sample of the ventral nail plate may be taken.
A No. 15 blade may also be used
to remove a specimen from the nail surface in white superficial onychomycosis.
Specimens suspected of candidal
onychomycosis should be taken from the affected nail bed closest to the
proximal and lateral edges.
Nail fragments must be small
enough for examination under low power. Large pieces of nail plate may be
pulverized prior to microscopy by using a hammer or a nail micronizer.
Counterstains, such as chlorazol black E or Parker blue-black ink, may be used
to accentuate the hyphae. It is reported that drilling to obtain specimens and
taking the sample from a more proximal site yield better results.
Culture
Direct microscopy cannot
identify the specific pathogen involved in onychomycosis. A fungal culture must
be used to identify the species of organism. Non dermatophyte
molds may be resistant to the conventional therapy used for the more common
dermatophytes. Therefore, 2 types of growth medium should
be used, one with cycloheximide (dermatophyte test medium [DTM], Mycosel, or
Mycobiotic) to select for dermatophytes and one without cycloheximide
(Sabouraud glucose agar, Littman oxgall medium, or inhibitory mold agar) to
isolate yeasts and non dermatophyte molds.
Cultures should be
obtained from pulverized nail scrapings or clippings while the patient has
abstained from antifungal medication for at least 2 weeks.
Cultures are
incubated for three to four weeks and examined weekly. Fungal colonies are
judged on the basis of growth patterns, color and microscopic formation of
macro and microconidia or other typical growth features. If
growth is seen on both types of media, the infective agent is probably a
dermatophyte, whereas growth only on the cycloheximide-free medium indicates
that the infective agent may be an NDM. Additional special culture
media such as Potato Glucose Agar or Urea Agar may be needed to definitively
differentiate between dermatophyte species.
Diagnosis of NDM requires more than one laboratory analysis to show consistency of fungal growth. If NDM infection is present in the first culture, the patient should be re-examined on next visit and three separate samples should be taken from the affected nail. If NDM is confirmed in all three of the cultures taken, the diagnosis of NDM is considered established and appropriate treatment can be started.
Histologic Findings
Surgical
pathology testing for OM using PAS (periodic acid Schiff stain) is the
current Gold standard for the diagnosis of OM.
Histologic examination of the
nail is a very useful alternative to culture or KOH testing. Nail clippings may
be sent to the laboratory for diagnosis in a formalin-filled container, or, as
a last resort, an incisional nail biopsy (by punch or scalpel) may be performed
to help confirm the diagnosis. Staining in the laboratory should be performed
with periodic acid-Schiff stain (PAS) or methenamine silver stain to reveal
fungal elements.
For
histopathological examination, rather large nail clippings are taken, fixated
for 4-8 hours in formalin and then softened [using agents like Potassium
hydroxide (KOH), 5% trichloroacetic acid, 10% Tween- 40, or chitin softening
solution containing mercuric chloride]. Softened tissue sample are
fixed in 10% buffered phosphate formalin for 24 h, dehydrated and then
embedded. Semi-thin sections (5 microns) are taken using a microtome and
stained with periodic acid-Schiff (PAS), the procedure altogether taking about
24-48 hours.
A comparison of diagnostic
methods revealed that a nail biopsy and staining with PAS is the most sensitive
technique available to diagnose onychomycosis. Examining
formalin-fixed, PAS-stained specimens has a higher probability (a higher
negative predictive value) than KOH examination in determining that a patient
is disease free if the test results are negative.
PAS is found to
be the most sensitive single test for the diagnosis for OM with a sensitivity
of 82%, followed by culture (53%) and direct microscopy
(48%). Histopathology not only proves the presence of fungus within the
nail plate, but also gives a valuable clue to the level of invasion and its
arrangement. Staining with Grocott methenamine-silver (GMS) has been shown to
be qualitatively superior to PAS as it provides greater contrast between fungus
and surroundings thus making identification easier. However, the procedure is
more complex.
Histopathological examination is useful for
distinguishing between dermatophytes, yeast and NDM and allows for examination
of mycelia threads and spore morphology in detail. However, the time
required for the procedure is the disadvantage which needs to be overcome.
Hyphae are seen between the nail laminae
parallel to the surface and have a predilection for the ventral nail and
stratum corneum of the nail bed. The epidermis may show spongiosis and focal
parakeratosis, and there is a minimal dermal inflammatory response. In WSO, the
organisms are present superficially on the dorsal nail and display unique
“perforating organs” and “eroding fronds.” In candidal onychomycosis there is
invasion of pseudohyphae throughout the entire nail plate, adjacent cuticle,
granular layer, and stratum spinosum of the nail bed, as well as the
hyponychial stratum corneum. As in direct
microscopy, histopathologic diagnosis does not identify the species of
causative pathogen.
Newer
methods
Polymerase chain reaction (PCR
Polymerase chain reaction (PCR)
assays have been developed to detect fungal DNA from infected nails. A
highly sensitive nested PCR assay using species-specific primer pairs based on
the 28S ribosomal RNA gene has been developed. This methodology permits
detection of both dermatophytes and nondermatophytes.
Matrix-Assisted Laser Desorption/Ionization
Time-of-Flight Mass Spectrometry (MALDI-TOF MS)
This technique is based on the detection of
biochemical characteristics which are a result of the activity of mycological
infections or noninfectious diseases. These are represented by proteolytic
degradation products of native nail proteins. The technique
analyses the protein patterns of nail samples by using small amounts of
peptides derived from tryptic digests of collected samples. The peptide
patterns of affected samples are identified by comparison with known peptide
spectra from nail disorders stored in an already existing data base. The
technique does not require any living or nonliving fungal material to prove or
to rule out OM. It is also able to discriminate between OM and nonfungal nail
disorders offering a distinct advantage over the conventional methods of KOH
and culture which only prove or rule out presence of fungi. Observer
skill is less important compared to other newer methods, as the results depend
on software assisted analysis. The preparation of nail material is simple. The
method is also fast, with results available within 24 hours.
Phase contrast hard X-ray microscopy
This technique uses phase contrast microscopes
utilizing synchrotron radiation. Synchrotron radiation can provide a
precise image of an extremely small object because of its brightness and high
spatial resolution (upto 70 nm). Hence, it can precisely image the
internal structure of dermatology specimens. This helps in observing minute
structures without requiring fixatives or stains. Resolution is also
much improved. The major advantage with this technique of
microscopy is that, just like histopathology, it provides direct evidence of
fungal invasion of nail plate, showing that the fungi are pathogenic.
Dermoscopy
Dermoscopy is useful to
distinguish distal subungual onychomycosis from traumatic onycholysis. In
distal subungual onychomycosis, the proximal border of the onycholytic area is
jagged owing to the presence of yellow-white spikes that project into the
proximal nail plate. This patterned has been reported as the "aurora
borealis" pattern.

Differential
diagnosis
The destructive changes of the nail
plate and nail bed produced by dermatophytes can be mimicked closely by
psoriasis. Fine pitting of the dorsal nail plate is never produced by fungal
infections and strongly suggests psoriasis, as does the oil-drop sign away from
the free edge. Paronychia caused either
by bacteria or by Candida, usually affects the nail plate proximally and
laterally, while the free edge is often spared, at least initially. Conversely,
swelling of the nail fold is rare in dermatophyte infections, and purulent
discharge is never a feature of uncomplicated tinea unguium. Ringworm of the nails is rarely symmetrical,
and it is common to find the nails of only one hand affected. The skin of the
feet and of the palms should always be examined carefully. Nail clippings or
scrapings are essential, and direct microscopy should be carried out with great
care, as culture often fails with nail plate material. For this reason, it is
wise to sample any obvious skin lesions present, as these are usually infected
with the same organism and will be more likely to yield a positive culture.
Prognosis
The goals for antifungal
therapy are mycological cure and a normal looking nail. Mycological cure can be
evaluated at the end of treatment, while clinical cure requires several more
months owing to slow nail growth.
Clinical trials have repeatedly
demonstrated higher efficacy for terbinafine compared with other antifungal
treatments.
Yellow streaks along the
lateral margin of the nail and/or presence of yellow onycholytic areas in the
central portion of the nail (dermatophytoma) are associated with a poor
response to treatment.
Residual nail changes persist
in most patients as a result of the frequent association of onychomycosis with
traumatic toenail dystrophies.
Onychomycosis caused by molds,
particularly Fusarium species,
are often not responsive to systemic therapy.
Recurrence (relapse or
reinfection) of onychomycosis is not uncommon, with reported rates ranging from
10-53%.
Fungal infections of the
fingernails have a much more favorable prognosis than toenail infections.
Treatment
Treatment of onychomycosis depends on the
clinical type of the onychomycosis, the number of affected nails, the severity
of nail involvement, associated tinea pedis, along with efficacy
and potential adverse effects of any treatment regimen. While it seems
reasonable not to treat minimal nail involvement, concurrent tinea pedis should
always be treated, particularly in the setting of diabetes mellitus, to prevent
cellulitis. A systemic treatment is always required
in proximal subungual onychomycosis and in distal lateral subungual
onychomycosis involving the lunula region. White superficial onychomycosis and
distal lateral subungual onychomycosis limited to the distal nail can be
treated with a topical agent. Because the rate of recurrence remains high, even
with newer agents, the decision to treat should be made with a clear
understanding of the cost and risks involved, as well as the risk of recurrence.
Photodynamic therapy and lasers may represent future treatment options.
Medications for onychomycosis
can be administered topically or orally. A combination of topical and systemic
treatment increases the cure rate. Adjunctive surgical measures may also be
used.
Topical therapy for
onychomycosis is as follows:
·
Ciclopirox olamine 8% nail lacquer solution
·
Amorolfine 5% nail lacquer solution
·
Efinaconazole 10% topical solution (the first FDA-approved
topical triazole for toenail onychomycosis)
·
Tavaborole 0.5% topical solution, an oxaborole solution
(boron-containing compound)
·
Can be used in WSO and DLSO limited to the distal nail
·
Should be limited to cases involving less than half of the
distal nail plate or for patients unable to tolerate systemic treatment
·
Topical treatments may be useful to prevent recurrence in
patients cured with systemic agents
Oral therapy for onychomycosis
is as follows:
·
Terbinafine
·
Itraconazole
·
Fluconazole and posaconazole are off-label
alternatives
·
Systemic treatment is always required in PSO and in DLSO
involving the lunula region
Nonpharmacologic approaches
include the following:
·
Laser treatment
·
Photodynamic therapy
·
Mechanical, chemical, or surgical nail avulsion
·
Chemical removal with a 40-50% urea compound in patients with
very thick nails
·
Removal of the nail plate as an adjunct to oral therapy
Laser treatment can be combined
with topical antifungals.
Topical antifungals
In those patients involving
less than half of the distal nail plate, superficial white onychomycosis and/or
contraindication for systemic treatment, topical therapy should be considered. Agents commonly used include ciclopirox olamine 8%,
amorolfine, and efinaconazole 10% nail solutions. Topical treatments alone are generally unable
to cure onychomycosis because of insufficient nail plate penetration.
Ciclopirox and amorolfine solutions have been reported to penetrate through all
nail layers but have low efficacy when used as monotherapy. They
may be useful as adjunctive therapy in combination with oral therapy or as
prophylaxis to prevent recurrence in patients cured with systemic agents.
Ciclopirox 8% lacquer applied to the
nail and surrounding skin at bedtime daily for 7 days and then removed with rubbing
alcohol and repeat the application for 48 weeks achieved mycologic cure in
29%–36% of cases and clear nails (clinical cure) in 7% of mild to moderate
cases of onychomycosis caused by dermatophytes. Despite its much lower efficacy
compared with oral antifungal agents, use of topical ciclopirox avoids risk of
drug interactions. Amorolfine
is mainly used as a treatment for onychomycosis in the absence of matrix
involvement in the form of 5% nail lacquer applied after abrading the nail once
or twice weekly until the regeneration of nail (approximately 6 months in
fingernail and 12 months in toenail onychomycosis). It
is the first member of a new class of antifungal drugs, the morpholine
derivatives, which show activity against yeasts, dermatophytes and molds that
cause onychomycosis. Amorolfine may have higher mycologic cure rates (38%–54%
after 6 months of treatment) compared to ciclopirox lacquer.
New topical antifungals treatments
Efinaconazole
It is a topical triazole
antifungal agent. It inhibits fungal lanosterol 14α-demethylase involved in the
biosynthesis of ergosterol, a constituent of fungal cell membranes. E‑ naconazole (Jublia
10% solution) is a topical imidazole active against dermatophytes and yeasts.
It received FDA approval in 2014. Having a low affinity for keratin, this drug
is able to penetrate the nail plate easily and selectively target pathogenic
fungi. Despite having a higher molecular weight than ciclopirox, its low
surface tension is thought to allow better penetration. Once within the nail,
efinaconazole is observed to have a better efficacy than what is noted for
ciclopirox. Studies showed that a single application of efinaconazole to the
hyponechium was able to reach the site of infection at the nail bed and
underside of the nail plate. Studies showed that the drug was able to penetrate
the nail without disrupting the polish, resulting in a similar concentration as
seen in control specimens free of polish.
Tavaborole
Tavaborole is boron based topical antifungal containing oxaborole molecules
approved in 2014. It is available as 0.5% topical
solution.
The increased affinity for fungal enzymes allows the drug
to be selective against the pathogen without interfering with host protein
synthesis. It is indicated for the treatment of onychomycosis caused by T.
rubrum and T. mentagrophytes; however, it is also effective against an array of
less commonly encountered pathogens, such as yeast. The low molecular weight of
tavaborole allows for easy nail penetration. Drug levels in the nail remain
high even at three months after treatment cessation. Using liquid
chromatography and mass spectrometry, ex-vivo cadaveric nail studies showed
significantly higher drug penetration of tavaborole compared to ciclopirox.
Moreover, studies evaluating the effects of nail polish on drug penetration
determined that the presence of nail polish did not hinder the transungual
delivery of tavaborole and might even enhance it. Despite the concern of
boron-related toxicity, tavaborole appears to have an excellent safety profile,
showing no cytochrome enzyme inhibition and negligible plasma levels after
topical use.
Auriclosene
Auriclosene is a broad-spectrum antibacterial and
antifungal agent belonging to a family of compounds known as aganocides.
Current clinical studies are focusing mainly on the treatment of impetigo,
conjunctivitis, and urinary catheter infections. However, preclinical studies
have assessed its utility in the treatment of onychomycosis; an in-vitro
evaluation on a cadaveric model utilized nanoemulsion lacquers and gel
formulations to assess the growth inhibition of dermatophytes, which showed
significant drug penetration and fungal eradication.
ME1111
ME1111 is a fungicidal compound effective against
dermatophytes, reaching sufficiently high concentrations in the nail to
overcome the minimum inhibitory concentration (MIC) of these organisms. The
ability of this drug to exert antifungal activity in the presence of keratin
has not been assessed. However, the effect of ME1111 showed selective toxicity
to the fungal organisms. Phases I and II clinical trials assessing the
pharmacokinetics and safety of ME1111 were recently completed, but results have
not been published yet.
Luliconazole
Luliconazole is an imidazole antifungal with an added
ketone dithioacetate component. In spite of its higher molecular weight, a
modified molecular structure endows this novel antifungal with lower keratin
affinity and, in turn, potentially improved potency. This drug is FDA-approved
in a cream formulation for the treatment of fungal infections of the skin.
Studies pertaining to onychomycosis used solutions of 5% applied daily for 48
weeks and assessed outcomes at the end of the treatment course; at this concentration,
randomized control studies showed similar efficacy for Luliconazole and other
approved topical treatments.
Systemic Therapy
An oral antifungal is required for onychomycosis
involving the matrix area, or when a shorter treatment regimen or higher chance
for clearance or cure is desired. Selection of the antifungal agent should be
based primarily on the causative organism, the potential adverse effects, and
the risk of drug interactions in any particular patient.
The newer generation of oral antifungal
agents (itraconazole and terbinafine) has replaced older therapies in the
treatment of onychomycosis. They offer shorter treatment
regimens, higher cure rates, and fewer adverse effects. Fluconazole and the new
triazole posaconazole (both not approved by the US Food
and Drug Administration [FDA] for treatment of onychomycosis) offer an
alternative to itraconazole and terbinafine. The efficacy of the newer
antifungal agents lies in their ability to penetrate the nail plate within days
of starting therapy. Evidence shows better efficacy with terbinafine than with
other oral agents. To decrease the adverse effects and duration
of oral therapy, topical treatments and nail avulsion may be combined with oral
antifungal management
Terbinafine is fungistatic and
fungicidal against dermatophytes, Aspergillus, and less so against
Scopulariopsis. Terbinafine is not recommended for candida onychomycosis since
it demonstrates variable efficacy against Candida species. A course of
terbinafine 250 mg daily for 6 weeks is effective for most fingernail
infections, while a minimum 12-week course is required for toenail infections.
Most adverse effects are gastrointestinal such as diarrhea, nausea, taste
disturbance, and elevation of liver enzymes. Evidence suggests that a 3-month
continuous regimen of terbinafine is the most effective oral treatment for
onychomycosis of the toenails available today. Clinical cure rates are
approximately 50%, although the success rate is lower in patients over 65
years.
Itraconazole is fungistatic against
dermatophytes, nondermatophyte molds and yeasts. Safe and effective schedules
include pulse dosing with itraconazole 400 mg daily for 1 week per month or a
continuous dose of 200 mg daily, both of which require 2 months or 2 pulses of
treatment for fingernails and at least 3 months or 3 pulses for toenails.
Itraconazole is dosed by weight in children at 5 mg/kg/day. Elevated liver
enzymes occur in 0.3%–5% of patients during therapy and return to normal within
12 weeks of discontinuation. Although itraconazole has a broader spectrum of
activity than terbinafine, studies have shown a significantly lower rate of
cure (about 25% vs. 50%) and higher relapse rate (about 50% vs. 20%) with
itraconazole compared with terbinafine. Fluconazole is fungistatic against
dermatophytes, some nondermatophyte molds, and Candida. The usual regimen for
fluconazole is 150–300 mg once weekly for 3–12 months.
Some, possibly 15% of patients, fail
to respond to these drugs, and there is a strong clinical impression that results
are much better in younger patient in that has faster linear nail growth and
relative absence of coexisting ischemic or traumatic dystrophy is probably
important factors. Poor peripheral circulation seems to have an adverse effect
on treatment.
Avulsion of the nail or removal of
the infected areas with a drill or burr as adjuncts to antifungals is
occasionally valuable. The use of 40% urea cream under occlusive dressing is an
alternative approach to treatment, particularly in oral treatment failures. The
addition of the imidazole, 1% bifonazole, to the urea paste has produced good
responses in some patients with involvement of the entire nail plate. When a
single great toenail is infected, these procedures are worthy of serious
consideration. The use of combined treatment
with either terbinafine or itraconazole with amorolfine may be more effective
than oral therapy alone.
Although
“cure” rates of up to 80% (or higher with prolonged therapy) have been reported with newer
antifungal drugs (itraconazole, fluconazole and terbinafine), recurrent
disease, especially in toenails, is common. Preventive measures include
breathable footwear and cotton socks, antifungal or absorbent powders, frequent
nail clipping and avoiding re-exposure (e.g. not going barefoot in locker
rooms). Old shoes often harbor large numbers of infectious organisms and should
be discarded or treated with disinfectants or antifungal powders.
|
INDICATORS OF MORE
SEVERE ONYCHOMYCOSIS WITH A POOR RESPONSE TO TREATMENT |
|
|
Nail factors |
·
Subungual
hyperkeratosis >2 mm thick (Measurement
of nail plate plus nail bed). ·
Significant
lateral involvement ·
Dermatophytoma
(Streak or patch representing a subungual pocket of densely
packed hyphae; removal prior to initiating antifungal therapy can be
helpful). ·
>50%
involvement of nail bed ·
Slow nail
growth rate ·
Total
dystrophic onychomycosis ·
Matrix involvement |
|
Patient factors |
·
Immunosuppression ·
Peripheral
arterial disease ·
Poorly
controlled diabetes mellitus |
Treatment ladder
First line
·
Oral terbinafine 250 mg/day for 6
weeks for fingernails, for 3 months for toenails
Or
·
Itraconazole 400 mg/day for 1 week,
monthly for 2–3 months for fingernails, for 3–4 months for toenails
Second line
Topical treatment with amorolfine or
ciclopirox olamine can be used in mild infections affecting the distal nail
plate only or superficial white onychomycosis.
Guidelines
Summary
In 2014, the British
Association of Dermatologists published updated evidence-based guidelines for
the management of onychomycosis. Treatment
recommendations are given for both adults and children (ages 1-12 y).
Adult systemic treatment recommendations are as follows:
·
Terbinafine as first line of treatment for dermatophyte
onychomycosis and generally preferred over itraconazole; not recommended for
patients with active or chronic liver disease (level A)
·
Itraconazole as first line of treatment for dermatophyte
onychomycosis (level A)
·
Fluconazole may be a useful alternative in patients unable to
tolerate terbinafine or itraconazole (level B)
·
Griseofulvin is no longer a treatment of choice owing to lower
efficacy and higher relapse rates compared with terbinafine and itraconazole
(level C)
·
Combination treatment recommended if response to topical
monotherapy is likely to be poor (level D)
Adult topical treatment recommendations are as follows:
·
Amorolfine or tioconazole are useful for superficial and distal
onychomycosis (level D)
·
Ciclopirox is useful for superficial and distal onychomycosis
and for patients in whom systemic therapy is contraindicated (level D)
Adult other treatment recommendations are as follows:
·
Surgical avulsion, debridement alone, and photodynamic therapy
(PDT) not recommended
Children systemic treatment recommendations are as follows:
·
Terbinafine as first line of treatment for dermatophyte
onychomycosis and generally preferred over itraconazole (level A)
·
Itraconazole is first line of treatment for dermatophyte
onychomycosis (level A)
·
Fluconazole considered as second line if itraconazole and
terbinafine contraindicated or not tolerated (level B)
·
Griseofulvin considered as second line if itraconazole and
terbinafine contraindicated or not tolerated (level C)
Steroid‐modified tinea (tinea
incognita)
Introduction
These are ringworm infections
modified by corticosteroids (systemic or topical) prescribed for some pre‐existing pathology or given
mistakenly for the treatment of misdiagnosed tinea.
Normally, the clinical diagnosis of
tinea depends heavily on the inflammatory changes involved. This inflammatory
response may be almost totally suppressed by corticosteroids, systemic or
topical. At the same time, it is probable that the resistance to infection
mediated by the immune response, especially the cell‐mediated response, is diminished by
corticosteroids. In this situation, the patient suffers doubly: the infection
is less likely to be diagnosed, and the patient has been rendered more
susceptible to that infection.
With patients on systemic steroids
(perhaps treated with additional immunosuppressive agents or irradiation), the
degree of modification is often minor, but even in these cases it may be
sufficient to mislead, especially on the face. With topical steroids, the
degree of modification can be profound. The usual sites where this problem
occurs are the groins, lower legs, face and hands, but tinea circinata
elsewhere may be steroid treated.
Clinical
features
History
The
history is characteristic. The patient is often satisfied initially with the
treatment. Itching is controlled and the inflammatory signs settle. But there
is a relapse on stopping treatment, with varying rapidity. Further applications
bring renewed relief and the cycles are repeated. In the groins, the patient
may develop few persistent nodules, which become insuppressible by the steroid
preparation.
Presentation
Typically,
the raised margin is diminished. Scaling is lost and the inflammation is reduced
to a few nondescript nodules. Often, a bruise‐like brownish discoloration is seen, especially in the
groins. On the face, the picture may be modified by superimposed perioral
dermatitis with papules and tiny pustules. Steroid‐modified eyelid infection may
closely resemble a sty. With chronic use, atrophy, telangieciectasia and, in
the groins and axillae, striae are likely to be observed. In some cases,
concentric rings of erythema are seen among the atrophy and telangiectasia.
Presumably, these represent waves of fungal growth. The eruption remains
localized but, especially in E. floccosum infections, it spreads more
widely. Strong fluorinated steroids seem most likely to produce this syndrome,
but even 1% hydrocortisone cream can, on occasions, modify tinea to a confusing
extent.
Differential
diagnosis
The
differential diagnosis of other steroid‐modified infections in the groin, particularly candidosis,
must be considered, and these may be indistinguishable without cessation of
therapy and mycological investigations.
Investigations
Scrapings
may be difficult to obtain in a patient who is currently applying a steroid
cream, but if he or she stops it for a few days an upsurge of inflammation with
marked scaling often occurs, making clinical diagnosis easier and facilitating
the taking of scrapings. In such samples, fungal mycelium is usually abundant
but scrapings taken while steroids are still being applied may show very few
fungal elements, unless a fluorescent whitener is used.
Treatment
Whatever site is affected, it is
often best to treat steroid‐modified
ringworm with oral therapy, allowing a few applications of topical steroid to
continue until the terbinafine or itraconazole has begun to take effect. It is
wise to use 1% hydrocortisone cream or at least a weaker steroid than that
originally prescribed, and also to warn the patient about a possible rebound in
spite of these measures. Follow‐up
to ensure steroid cream has been stopped and cure obtained is mandatory.
Dermatophytide reactions
Definition
This is a non‐infective inflammatory cutaneous
eruption representing an allergic response to a distant focus of dermatophyte
infection.
A local DTH response to systemically absorbed fungal antigen is observed.
Predisposing
factors
The
essential criteria required for the diagnosis of an ide reaction to a
dermatophyte infection are the following:
1.
Proven dermatophyte infection, which
usually becomes highly inflamed before the appearance of the secondary rash.
2.
A distant eruption, which is
demonstrably free of ringworm fungus.
3.
Spontaneous disappearance of the
rash when the ringworm infection settles, with or without treatment.
4.
The morphology of the ide eruption
should match one of the following well‐recognized types.
Clinical
features
1.
A widespread eruption of small
follicular papules grouped or diffusely scattered. The eruption is symmetrical,
usually pronounced on the trunk, but in severe cases extending down limbs, even
at times covering the face. Sometimes the follicular papules are topped by
horny spines. The common cause of this type of ide reaction is a scalp ringworm
kerion, typically caused by T. verrucosum. On occasions, T. tonsurans
and M. audouinii may be responsible, when they produce inflamed
ringworm. Treatment of the original ringworm lesion may play a part in
initiating the process.
2.
A pompholyx‐like ide affecting the web spaces
and palmar surfaces of the fingers, the palms and sometimes the dorsal surfaces
of the hands. This eruption is characteristically associated with an acutely
inflammatory tinea pedis, which may have arisen spontaneously or as a result of
inappropriate treatment. The palmar and web space skin may be covered with
papules or vesicles. On occasions, bullae or pustules may occur. Clinically,
this is indistinguishable from a constitutional eczema of the pompholyx
variety, and the diagnosis of a dermatophytide in this clinical situation
demands rigorous application of the criteria outlined above.
DIAGNOSTIC PROCEDURES
OF DERMATOPHYTOSIS
The clinical diagnosis of a dermatophyte infection can be
confirmed by microscopic detection of fungal elements, by identification of the
species through culture, or by histologic evidence of the presence of hyphae in
the stratum corneum. In addition, fluorescence patterns under Wood's light
examination may support a clinical suspicion.
Microscopic Examination
Although microscopic evaluation of potassium hydroxide
(KOH)-treated samples does not allow for speciation or characterization of the
susceptibility profile, it is used as a quick and inexpensive bedside tool to
provide evidence of dermatophytosis.
Scale from skin should be collected by scraping the
involved area with a dull edge outward from the advancing margins. Full
thickness nail clippings should involve the dystrophic portion, as proximal
from the distal edge as possible without causing injury. Hairs should be
plucked (not cut). The specimen is then placed on a glass slide and adds 1–2
drops of a 10%–20% KOH solution and covered with a cover slip and
then examined under low power microscope. Slightly warming the slide with a low
intensity flame allows better penetration of the KOH solution into keratin.
All the dermatophyte species
appear identical in skin and nail samples. Septate and branching hyphae
without constriction at the
branching point may be visualized under microscopic examination with
10%–20% KOH preparation. The hyphae
are very even in diameter along their length and regularly septate. In some
specimens the hyphae fragment to form arthroconidia, which disarticulate when
mature, and may then round up and increase notably in size. These germinate to
produce true hyphae. The chlorazol black E stain can help to highlight fungal elements
in KOH preparations. Use of calcofluor, a fluorescent stain specific for the
chitin in the fungal cell wall, and examination with a fluorescent microscope
can also demonstrate fungi (apple-green fluorescence).
Hair invasion results in
three distinct patterns: ectothrix, arthrosporic endothrix and favus
endothrix and these are readily distinguishable by the arrangement and the
size of the fungal elements. When trying to determine whether infection is
endothrix or ectothrix, it is useful to note that the pigment in the hair
clearly delineates the edge of the hair shaft, and can be used as a marker to
judge whether the fungus is entirely confined within the hair or has formed an
ectothrix sheath of arthroconidia on the surface. Low-power
microscopy will reveal: (1) Ectothrix—small or large arthroconidia forming a
sheath around the hair shaft, (2) Endothrix—arthroconidia within the hair
shaft, or (3) Favus endothrix —hyphae and air spaces within the hair shaft.
Because KOH examination may yield false-negative results
in up to 15% of cases, patients suspected of having dermatophytosis on clinical
impression should be treated. Culture confirmation should be considered
whenever systemic treatment is warranted, such as in the case of tinea capitis.
Culture
Sabouraud's dextrose agar (SDA) is the most commonly used
isolation medium for dermatophytes and it serves as the medium on which most
morphologic descriptions are based. Elimination of contaminant molds, yeast and
bacteria is achieved by the addition of cycloheximide and chloramphenicol (+/−gentamicin) to the
medium making it highly selective for the isolation of dermatophytes. The
development of colonies can take 5–7 days in the case of Epidermophyton
floccosum and up to 4 weeks for Trichophyton verrucosum. Cultures are incubated
at room temperature (20°C–25°C) for at least 4 weeks before being finalized as
no growth.
Dermatophyte test medium (DTM) is an alternative
isolation medium that contains the pH indicator phenol red. The medium turns red when
dermatophyte proteolytic activity increases the pH to 8 or above, and it
remains amber with the growth of most saprophytes. Nondermatophyte acidic
byproducts turn the medium yellow.
Histopathology
Skin biopsy is not often employed in the workup of
typical dermatophytoses. Localized cutaneous eruptions suspected to represent
dermatophytosis with equivocal KOH examination are often treated despite the
lack of confirmation. Biopsy may confirm the diagnosis when a systemic agent is
being considered for treatment of a recalcitrant or more widespread eruption.
Biopsy may be used to aid in the diagnosis of Majocchi's granuloma in which KOH
examination of scale on the surface may more often be negative. Biopsy is also
sometimes useful in confirming the presence of hyphae involving hair shafts on
the scalp in tinea capitis, although culture is necessary to allow speciation
of the pathogen. When present, hyphae may be appreciated in the stratum corneum
on hematoxylin and eosin staining. However special stains, most commonly
periodic acid-Schiff (PAS) and methenamine silver stains, highlight
hyphae that may otherwise be subtle in appearance on routine staining. Whereas
culture is the most specific test for onychomycosis, PAS examination of nail
clippings is the most sensitive and it obviates the need to wait weeks for a
result.
Wood's Light Fluorescence
Examination of involved hair bearing areas, such as the
scalp or beard, with a Wood's lamp (365 nm) may reveal pteridine fluorescence
of hair infected with particular fungal pathogens. Hairs that fluoresce should
be selected for further examination, including culture. While ectothrix
organisms M. canis, M. audouinii and M. ferrugineum will fluoresce yellow-green
on Wood's light examination, the endothrix organisms T. tonsurans and T.
violaceum will not fluoresce.
Dermoscopy
The comma hairs, which are slightly curved,
fractured hair shafts, and corkscrew hair shave been described as the
dermoscopic marker of tinea capitis. Broken and dystrophic hairs are also seen.
However, in tinea corporis, the involvement of vellus hair as seen on
dermoscopy is an indicator of systemic therapy.
Polymerase
chain reaction and nucleic acid sequence based amplification
These tests not only help in the rapid and
early diagnosis of infection but also help in determining drug resistance, and
include:
·
Uniplex PCR for direct dermatophyte detection in clinical samples:
A PCR for the direct detection of dermatophytes in skin scales is available as
in-house PCR-ELISA assay which separately identifies numerous dermatophyte
species. In a pilot study, the sensitivity and specificity of the test compared
to cultures was 80.1% and 80.6%
·
Multiplex PCR for fungal detection in dermatophytes: Commercially
available multiplex PCR tests enable simultaneous amplification of 21
dermatomycotic pathogens with subsequent DNA detection by means of agarose gel
electrophoresis.
Common Laboratory Dermatophyte Identification Methods
|
Laboratory Test |
Method |
Function |
Findings |
|
Potassium hydroxide preparation |
Scales from the advancing border, subungual debris, or
affected hair removed and placed on a glass slide. KOH 10% dropped on
specimen and covered with a cover slip. The undersurface of the glass slide
may be gently heated with a low-lit flame. |
KOH solution and gentle heating softens keratin and
highlights the dermatophyte. |
Long narrow septated and branching hyphae |
|
Culture |
Sabouraud medium (4% peptone, 1% glucose, agar, water) |
Facilitates growth of dermatophytes |
Microscopic morphology of microconidia and
macroconidia, along with culture features including surface topography and
pigmentation. |
|
Modified Sabouraud medium (addition of chloramphenicol, cycloheximide, and gentamicin) |
Facilitates growth of dermatophytes and inhibits growth
of non-Candida albicans, Cryptococcus, Prototheca species, P. werneckii,
Scytalidium species, Ochroconis gallopava |
||
|
|
|
|
|
|
Histolopathology special stains: periodic acid-Schiff
and Grocott's methenamine silver |
Tissue may be obtained by skin or nail biopsy
techniques |
Stains fungal cell wall to detect fungal elements in
tissue sections |
Pink (PAS) or black (GMS) fungal elements noted
in the stratum corneum |

Proper collection of skin, hair, and nails
is important. Following these simple guidelines will help the clinician to
achieve the most accurate diagnosis.
Differential diagnosis
Careful
clinical examination is the first and most important step in diagnosing
dermatophyte infections. Because many other conditions can mimic
dermatophytoses, KOH examination and/or culture are often necessary to confirm
the diagnosis.
Colonial
morphology, microscopic examination of conidia (the asexual propagules formed de
novo by the fungus), allow precise identification of the dermatophyte. The
presence or absence of microconidia (usually small and unicellular) and
macroconidia (usually larger and multicellular) and the typical features of
each (such as shape and cell wall texture) remain fairly consistent among
genera. Other distinguishing microscopic features include the identification of
arthroconidia (infective fungal elements) and chlamydoconidia. Sometimes,
conidia may not be present in culture (“sterile” organism), and the hyphal
patterns (spiral, pectinate, antler, racquet, and nodular bodies) may be
important in identification of the organism. The color, texture and topography
of the colony are features that are unique to a particular species.


Management
Multiple topical and systemic antifungal agents are
available to treat dermatophytoses of skin, hair and nails.
Topical
antifungals are the first-line treatment for many patients with uncomplicated,
localized or mild cutaneous dermatophyte infections. Patients should be
counseled on the rule of two, i.e. topical antifungal to be applied 2 cm beyond
the margin of lesion twice a day for at least 2 weeks beyond clinical
resolution. The major potential adverse reaction is irritant (or, occasionally,
allergic) contact dermatitis, usually from the alcohols or other components in
the vehicle. Systemic antifungal therapy, although associated with both a
higher incidence of side effects including potentially severe adverse reactions
and the potential for drug–drug interactions, is typically required for
infections involving hair bearing skin such as tinea capitis and tinea barbae,
and nails ( tinea unguium) and is also needed for infections involving
extensive areas of skin, or associated with excessive inflammatory reactions.
The newer oral azoles, such as fluconazole or itraconazole and terbinafine, are
now the preferred oral treatments for extensive or severe dermatophytosis
rather than griseofulvin. The adjunctive use of topical products containing
glycolic acid, lactic acid or urea may help to reduce the amount of
hyperkeratosis in infections such as tinea manuum and tinea pedis.

ANTIFUNGAL targets. (a) Antifungal targets on the fungal cell. (b) Influence of individual active substances on ergosterol biosynthesis
Oral antifungal drugs
Terbinafine
Terbinafine is a member of the allylamine
antifungals that act by the inhibition of squalene epoxidase in the formation
of the fungal cell membrane. This enzyme acts at an early stage in membrane
biosynthesis, and the accumulation of squalene is thought to destabilize the
cell membrane. The two main antifungal compounds are naftifine and terbinafine.
Both are active in vitro against dermatophytes in addition to other
fungi; terbinafine is also active against Sporothrix schenckii, some Aspergillus
species and Histoplasma capsulatum. The drug is fungicidal rather than
fungistatic. Although it is not licensed for use in children, it has been
widely used off‐label
in this group of patients. Terbinafine can be given topically or orally. When
given orally, it is rapidly taken up into the stratum corneum and it persists
in nails at high concentrations for several months. These may exceed the
minimum inhibitory concentration 80 days after the end of therapy. Terbinafine
is given orally in a dosage of 250 mg/day. It has produced rapid and long‐lasting remissions in nail disease and
persistent tinea pedis, as well as tinea corporis. A smaller tablet form of 125
mg is available for the treatment of children. There are few drug interactions
reported for terbinafine, and side effects are uncommon. The spectrum of side effects includes headache,
nausea (usually in the first week; apply medication in the evening), and
(rarely) usually reversible taste loss. Terbinafine can worsen psoriasis or
provoke it de novo (usually within the first 4 weeks of treatment), and
drug-induced subacute-cutaneous LE can also occur, especially if risk factors
(pre-existing connective tissue diseases) are present. Hepatic reactions,
although reported, are exceptionally rare. Drug rashes including erythema
multiforme or toxic epidermal necrolysis are also seen on occasion.
Itraconazole
This is an orally active azole of
the triazole series. It has similar activity to ketoconazole, but without the
risk of hepatotoxicity. Its mode of action is through the inhibition of the
cytochrome P450‐dependent
demethylation stage in the formation of ergosterol on the fungal cell membrane.
It is active in vitro against all the main superficial fungal pathogens
including Candida albicans, pityriasis versicolor, as well as a wide
range of fungi that cause deep infections such asaspergillosis, histoplasmosis
and cryptococcosis. Itraconazole rapidly penetrates to the outer stratum
corneum and is also found in sebum. It is avidly bound to keratin‐containing tissues, and in nails,
for instance, may persist long after cessation of therapy. It has been shown
that after 3 months of 200 mg/day itraconazole, levels in the toenail persist
for up to 6 months. This feature allows a range of different dose regimens. The
initial treatment first described involving 100 mg/day itraconazole have been
superseded by higher or intermittent (pulsed) therapy. The currently preferred
regimen uses 400 mg/day, given as two daily doses of 200 mg. In tinea corporis,
1 week of therapy is sufficient, and in tinea pedis, 2 weeks. For
onychomycosis, a regimen of 400 mg/day for 1 week every month for 3 months is
usually given. Occasionally, longer periods of treatment are needed. It is
effective in tinea capitis also. There is some evidence that its absorption is
impaired in the presence of phenobarbital. It also interacts with coumarin
anticoagulants, ciclosporin, rifampicin, digoxin and statins. Side effects are uncommon
and mainly consist of nausea and abdominal discomfort. Hepatic reactions are
exceptional and liver function should be monitored if it is used for longer
than 1 month. It has been associated with heart failure and cardiac arrhythmias
in those at risk.
Fluconazole
Fluconazole is an orally active
triazole antifungal used for the treatment of dermatophyte infections (tinea),
pityriasis versicolor and mucocutaneous candidosis and also systemic mycoses.
In dermatophytosis it is given in a regimen of 150 mg/week for 2–3 weeks for
tinea corporis and tinea cruris, and somewhat longer for dry‐type tinea pedis. It is also
reported to be effective given in weekly doses in onychomycosis. There are
fewer interactions than with itraconazole but, like the latter, side effects
are rare and mainly confined to gastro‐intestinal discomfort. However, drug resistance in Candida
species, particularly C. krusei and C. glabrata, has been
described. There is also C. albicans resistance in some patients, particularly
in those with HIV/AIDS. It should be used with caution in those at risk of
cardiac arrhythmias.
Treatment of dermatophytosis
|
Disease |
Topical Treatment |
Systemic Treatment |
|
Tinea capitis |
Only as adjuvant Selenium sulfide 1% or 2.5% Zinc pyrithione 1% or 2% Povidone iodine 2.5% Ketoconazole 2% |
Adults: · Terbinafine, 250 mg/day × 2–4 weeks · Itraconazole 200mg/day × 2–4 weeks · Fluconazole, 6 mg/kg/day × 3-6 weeks Children: · Terbinafine daily x 2-4 weeks Weight < 20 kg = 62.5 mg/day Weight 20-40 kg = 125 mg/day Weight > 40 kg = 250 mg/day · Itraconazole, 5 mg/kg/day (maximum
200mg) × 2–4 weeks |
|
Tinea barbae |
Only as adjuvant Topical antifungals |
· Terbinafine, 250 mg/day × 2–4 weeks · Itraconazole, 200 mg/day × 2–4 weeks · Fluconazole, 200 mg/day × 4–6 weeks |
|
Tinea corporis/cruris |
Allylamines Imidazoles |
Adults: · Terbinafine, 250 mg/day × 2–4 weeks · Itraconazole, 200 mg/day × 1 week · Fluconazole, 150–300 mg/week × 4–6
weeks Children: · Terbinafine daily × 2 weeks (as for
T. capitis) · Itraconazole, 5 mg/kg/day (maximum
200mg) × 1 week |
|
Tinea pedis/manuum |
Allylamine Imidazoles |
Adults: · Terbinafine, 250 mg/day × 2 weeks · Itraconazole, 200 mg twice daily × 1
week · Fluconazole, 150 mg/week × 4-6 weeks Children: · Terbinafine daily × 2 weeks (as for
T. capitis) · Itraconazole, 5 mg/kg/day (maximum
200mg) × 2 weeks |
|
Onychomycosis |
Amorolfine |
Adults: · Terbinafine, 250 mg/day × 6–12 weeks · Itraconazole, 200 mg/day × 2–3 months Or pulse 400mg/day x 1 week/month for 2-3 months · Fluconazole, 150–300 mg/week × 3–12
months Children: · Terbinafine daily × 6–12 weeks Weight < 20 kg = 62.5 mg/day Weight 20-40 kg = 125 mg/day Weight > 40 kg = 250 mg/day · Itraconazole 1 week/month for 2-3
months Weight < 20 kg =5 mg/kg/day Weight 20-40 kg = 100 mg/day Weight 40-50 kg = 200 mg/day Weight >50 kg = 200 mg twice daily · Fluconazole, 6 mg/kg/week × 3–6
months |
Treatment failures
Failure
of topical therapy
Most
failures of topical therapy are caused by inaccurate diagnosis or by
inappropriate use of topical therapy (e.g. in hairy areas) or because the
treatment is not used. Once or twice daily application for several weeks is
usually required for success. Many dermatoses respond, at least temporarily, to
any bland application, and imidazole compounds in particular have considerable
antibacterial properties.
Failure
of oral therapy
When
a patient fails to respond to terbinafine, fluconazole or itraconazole, the
following points should be checked:
1.
Is the diagnosis correct? If
necessary, repeat scrapings.
2.
Has the patient been taking the
tablets regularly?
3.
Is the patient taking any potentially
competitive drugs?
4.
In spite of taking them correctly,
is the patient failing to absorb the antibiotic? An estimation of itraconazole
levels, which is sometimes poorly absorbed, may be helpful.
5.
In some patients with onychomycosis,
poor penetration of drugs into defined linear streaks or nail edge areas of
nail plate infection may account for treatment failure. Surgical removal of
these abnormal nail areas, often after softening with urea ointment, may be
useful.
6.
Is there coexisting pathology such
as HIV/AIDS or arterial disease?
7.
Is a co‐pathogen or secondary infection
present? This should be considered in the feet and in the case of kerions, and
perhaps in groin infections too. In nails, the coexistence of non‐dermatophyte fungus should be
considered. Scopulariopsis brevicaulis, apart from causing infections of
the toenails in its own right, may coexist with Trichophyton rubrum or T.
interdigitale and seems, at least on occasions, to cause failure of
treatment. Nail removal may be indicated in this instance.
8.
Antifungal resistance. This
phenomenon is sufficiently uncommon among dermatophytes to make routine testing
unnecessary, but where treatment failure occurs without any other explanation,
it is possible to estimate the sensitivity of the causal organism. This should
be performed by a specialist laboratory. Apart from true resistance, tolerance,
in which the organism apparently becomes clinically resistant to the drug in
the tissues but is sensitive in vitro, may also, be important.
9.
Reinfection. As ringworm fungi can
frequently be isolated from the environment, when there are cases of ringworm
of the scalp, and from clothing after laundering, it is highly likely that
patients whose infection has been eradicated may be re infected from these
sources. Unfortunately, there is no proven way to avoid this.
Despite running through this
checklist, dermatologists may not come up with an adequate explanation for
treatment failure. In these situations, the use of one of the alternatives is a
logical further step.
(IADVL) task force against recalcitrant
tinea (ITART) consensus on the management of glabrous tinea (INTACT), 2020
Definitions
Glabrous tinea: Dermatophytosis involving the skin of any site, except
terminal hair-bearing areas of the scalp and face (tinea capitis/tinea barbae),
palms (tinea manuum), soles (tinea pedis) and nails (tinea unguium);
notwithstanding the true meaning of glabrous as “without hair”. It constitutes
tinea corporis, tinea cruris and tinea faciei, and may also include involvement
of hair bearing regions without invasion of hair by fungi.
Chronic
dermatophytosis: Presence of glabrous tinea for a duration
of six months or longer, continuous or recurrent, with or without treatment.
Duration was earlier considered to be more than one year.
Recurrent
dermatophytosis: Reoccurrence of the glabrous tinea after 4
weeks of stopping treatment following clinical cure but less than 6 weeks
Relapse: Relapse denotes the
occurrence of dermatophytosis (lesions), after a longer period of
infection-free interval (6–8 weeks) in a patient who has been cured
clinically.
Resistant
dermatophytosis: Failure to eliminate dermatophytosis
despite administration of one or more antifungal agents for an adequate dose
and duration, based on clinical judgment due to proven mycological resistance
to the drugs.
Naïve case: A patient with glabrous tinea who has not received any prior
treatment.
Corticosteroid
modified tinea: Glabrous tinea whose morphology is altered
due to topical or systemic corticosteroids, but is still recognisable or
diagnosable.
Tinea incognito: Glabrous tinea in which the morphology is markedly altered
due to the suppression of inflammation by corticosteroids or other
immunosuppressants such that it is not easily recognisable as tinea.
Over-the-counter (OTC)
medications: Medications purchased from a pharmacy
without prescription by a qualified healthcare professional
Clinical cure: Complete resolution of symptoms and signs with or without
post-inflammatory changes at the end of treatment
Mycological cure: Complete subsidence of symptoms and signs
with negative mycological reports (direct microscopy and/or culture) at the end
of the treatment.
BSA: The area of outstretched
palm from the wrist to the tip of the fingers can be considered roughly 1% of
the body surface area. Less than 3% can be counted mild, 3–10% as moderate, and
more than 10% as severe, in terms of the extent of involvement.
Recalcitrant
tinea infection: This is
a generic term that may refer to relapse, recurrence, persistence of infection,
chronic infection, corticosteroid-modified
and resistant cases, with poor or no response to standard treatment.
Trichophyton Rubrum Syndrome is defined as
(A) Skin lesions at the following four sites:
(1) Feet, often involving soles;
(2) Hands, often involving palms;
(3) Nails; and
(4) At least one lesion in another location other than (1) (2) or (3), except
for the groin.
(B) Positive microscopic analyses of potassium hydroxide preparations of skin
scrapings, in all four locations.
(C) Identification of Trichophyton rubrum by cell culture at
three of the four locations at least.
For diagnosis of TRS, the criteria (A) and (B) and (C) have to be fulfilled.
Laboratory diagnosis
Role of various laboratory methods in the
diagnosis of dermatophytosis
|
Principle |
Method |
Comments |
|
Direct
microscopic examination |
Direct
microscopy using potassium hydroxide mount and its modifications |
An
office procedure with relatively high sensitivity |
|
Should
be done whenever feasible, especially if there is diagnostic difficulty on
clinical examination |
||
|
Histopathology |
Histopathology
with special stain with periodic acid Schiff (PAS) stain |
Indicated
in suspected Majocchi granuloma or deep dermatophytosis |
|
Isolation
by culture and species identification |
Fungal
culture on Sabouraud’s dextrose agar |
Sensitivity
is low, but specificity is high; considered as the gold standard in the
diagnosis |
|
May
be performed whenever feasible for confirmation of clinical diagnosis and to
understand the epidemiological trends in a region |
||
|
Identification
of species and subspecies by molecular diagnostic methods |
Sequencing
of the internal transcribed spacer (ITS) region of the ribosomal DNA, Random
Amplified Polymorphic DNA (RAPD), Amplified Fragment Length Polymorphism
(AFLP), mitochondrial DNA (mt DNA) restriction analysis, Sequencing of
protein-encoding genes, polymerase chain reaction (PCR) fingerprinting. |
Requires
specially equipped laboratory with trained manpower |
|
Currently
utilised for research purposes but may find a place in conventional diagnosis
in future |
||
|
Identification
of species and subspecies by proteomic signature |
Matrix-assisted
laser desorption/ionization time of flight (MALDI-TOF) mass spectrometry |
Requires
specially equipped laboratory with trained manpower |
|
Currently
used for research purposes but may find a place in conventional diagnosis in
future |
||
|
Antifungal
sensitivity testing (AFST) |
Microbroth
dilution method |
Tedious
procedure requiring trained manpower |
|
Lack
of reference data on minimum inhibitory concentration (MIC) of antifungal
drugs used against dermatophytes. |
||
|
If
facilities are available, it should be considered whenever there is a strong
suspicion of antifungal resistance |
||
|
Identification
of mutation causing antifungal resistance |
Real
Time Polymerase chain reaction (RT PCR), Sequencing of DNA |
Requires
equipped laboratory with trained manpower; currently utilised for research
purpose |
|
Whenever
there is strong suspicion of antifungal resistance it may be considered |
Diagnosis of dermatophytosis has lately become more challenging,
with atypical morphological variants being more commonly seen, of which many
are attributable to topical corticosteroid abuse. When clinical diagnosis is
difficult, experts recommended direct microscopic examination as an office
procedure with potassium hydroxide (KOH) mount, a test with high sensitivity,
to confirm dermatophytosis. The specimen should be obtained by scraping the
lesion's active margin when present or from its scaly region and transported in
a sterile, thick dry black sheet of paper to the laboratory, if the facility is
not available in the outpatient clinic. It is advisable to perform a microscopic
examination of 10% KOH mount of skin scrapings in every case, for a better treatment
outcome and should be observed 15–30 min after
preparation, to improvise the sensitivity. Dermatophytes
are visualized as hyaline, long, branching, septate hyphae with/without
arthrospores. But direct microscopy does not help to identify the species. If
feasible, the organism can be isolated by culture in modified Sabouraud's
dextrose agar with antibiotics and cycloheximide, to understand the
epidemiological trends in a region and for possible therapeutic implications.
Macroscopic appearance of culture colony and microscopic morphological features
of the microconidia, macroconidia and other vegetative structures can help to
identify the various species
Histological diagnosis of
dermatophytosis is not done routinely but can be useful in diagnosis of unusual
clinical presentations like Majocchi granuloma and deep dermatophytosis.
Staining with periodic acid Schiff (PAS) stain can ease identification of
hyphae in tissue.
Antifungal susceptibility testing (AFST) studies to know the local
drug susceptibility patterns and molecular diagnostic techniques required for
the accurate identification of the dermatophyte species may be considered in
research institutes or if reference laboratories are available. However, there
was no consensus on the utility of real time polymerase chain reaction (RT-PCR)
and matrix assisted laser desorption/ionization time of flight mass
spectrometry (MALDI-TOF MS) in the current scenario, since these are relatively
new and the clinical implications are not known.
General measures
Consensus on points for counseling patients
with dermatophytosis
|
Points
for discussion with patients |
Expected
impact |
|
Current
scenario of dermatophytosis in India |
Patients
will understand the gravity of the situation and follow medical advice
accurately |
|
Taking
regular bath (at least once a day) |
Reduces
fungal load due to exfoliation of scales |
|
Wiping
the body dry (especially intertriginous area and toe clefts) |
Prevents
high moisture in those parts, minimizing chances of fungal colonization |
|
Regular
washing of clothes in hot water and drying in sunlight inside out |
Reduces
chances of re-infection from infected clothes |
|
Storing
and washing clothes of infected patients separately |
Reduces
chances of transmission to contacts and family members |
|
Regular
washing of bed linen (at least once a week) |
Minimizes
chances of re-infection from infected linen |
|
Avoidance
of sharing of fomites like clothes, towels and soaps with others |
Reduces
transmission to contacts and family members |
|
Avoidance
of synthetic tight garments |
Prevents
occlusion, maceration, friction and barrier dysfunction |
|
Avoidance
of wearing bands, threads, draw strings and rings |
Reduces
chances of re-infection from such infected materials |
|
Regular
mopping and cleaning of the house |
Reduces
chances of persistence of dermatophytes in the environment |
|
Losing
weight in obese patients |
Reduces
chances of intertriginous fungal infections |
|
Avoidance
of contact with pets |
May
reduce zoophilic infection and transmission |
|
Avoidance
of application of topical corticosteroids |
Reduces
chances of unusual presentations, diagnostic difficulty and treatment failure |
|
Strict
adherence to treatment |
Enhances
chances of complete cure and reduces recurrence |
|
Simultaneous
treatment of other infected house members and close contacts (prophylactic
treatment is not required) |
Reduces
chances of transmission to each other and recurrence |
|
Avoidance
of self-medication, over the counter(OTC) medications and sharing of
prescriptions |
Reduces
chances of inadequate treatment, topical corticosteroid misuse and treatment
failure |
Global warming has affected the climate in
India in the form of increased maximum temperatures, heat waves and less
rainfall. Indian Meteorological department data have shown an increase of 0.6°C
in the average temperatures between 1901-10 and 2009-18. The number of days
with maximum temperature exceeding 35°C in various cities in India has also
increased. A hot and humid climate favors the growth of dermatophytes, while
humidity can enhance penetration of fungi. In a study from Kerala done in 2016,
52% of patients with chronic dermatophytosis were manual labourers. About 64%
of patients were exposed to the sun for more than 3 hours a day and 68% had
reported excessive sweating. In another study, from Tamil Nadu, chronic
infection was associated with sun exposure for more than 3 hours daily.
Maintenance of personal hygiene is very important to avoid
acquiring dermatophytosis and in preventing its spread and persistence. After
every bath, the entire body surface, especially the body folds and toe clefts,
should be wiped well. Washing of clothes and bed linen in hot water at 60°C and
drying them in sunlight inside out may help prevent persistence of infection.
Since direct contact and fomites play a significant role in the spread of
infection, patients should be advised to avoid sharing of inanimate objects or
fomites (e.g., soaps, towels, clothes and bedding) with others, as these can be
responsible for transmission of infection. Washing the body surface with soap
and water removes fungal elements, emphasizing the need for regular bathing.
Use of synthetic tight dresses and occlusive footwear is linked to increased
prevalence of dermatophytosis. Tight, restrictive clothing can trap heat and
moisture, leading to a conducive environment for the growth of dermatophytes.
Hence, patients should be advised to avoid using synthetic or tight clothing
and should preferably use loose cotton clothes. Regular mopping and cleaning of
the house would also help to reduce the persistence of dermatophytes in the
environment.
Washing clothes in water at a temperature of 60°C or above
eliminates Trichophyton
rubrum. Exposure of infected socks to sunlight can reduce fungal
contamination as sunlight can act as a good disinfectant. Washing or storing
infected and non-infected clothes together can facilitate transmission of
infection. Hence the worn clothes of patients should be stored and washed
separately in hot water at 60°C and dried inside out in the sun. Similarly,
ironing of clothes may also be beneficial. Waistbands, wristbands and threads,
which aid the persistence of dermatophytes, are better avoided.
Obese patients should be advised to lose weight to prevent
recurrence of infection, especially in intertriginous areas like the groin. The
nails should be examined in all patients with dermatophytosis as they may act
as a focus for recurrent infection. Contact with pets should be avoided as they
can be potential sources of infection, although there appears to be no role of
pets in the current scenario.
Abuse of oral or topical corticosteroids frequently leads to
diagnostic difficulty (due to atypical presentations of dermatophytosis) and
treatment failures. Compliance to treatment is essential to achieve cure as
patients often use antifungal drugs irregularly or stop them on getting relief
from itching and achieving partial resolution. As infection among other family
members is very common in the current scenario, treatment of all infected
members simultaneously is necessary to avoid recurrences or persistence of
infection. Counseling patients about the course of disease, adherence to
treatment and to general measures and avoidance of corticosteroid abuse are
essential for treatment to be successful.
To conclude, experts agreed that patients
should be educated about personal hygiene, clothing, skin care, corticosteroid
abuse, adherence to general measures and compliance to treatment to ensure
successful outcome.
Pharmacological therapy
Since dermatophytes usually do not penetrate
the deeper layers of the skin, the host does not necessarily develop sufficient
immunity to ensure spontaneous healing. Spontaneous remission rarely occurs
even when the underlying cause has been eliminated. Therefore, every patient
with dermatophytosis requires topical and/or systemic antifungal therapy.
Tinea of the glabrous skin has been easily
amenable to short courses of standard antifungal agents, terbinafine and
itraconazole since the time these drugs were introduced. However, with
increasing incidence of inadequate response to treatment, high recurrence rate
and chronic infections, an extended duration of therapy is often needed. To
ensure compliance, antifungal therapy should be chosen keeping affordability in
mind.
Topical
therapy
Consensus points on topical
therapy in patients with glabrous tinea infections
|
Consensus point |
Justification/comments |
|
Topical therapy can be used as a standalone
or an adjuvant therapy |
Topical therapy attains high antifungal
concentration at the site of infection |
|
Antifungal preparation alone without any
corticosteroid or antibacterial component should be used |
Corticosteroid application can result in
treatment failure and local adverse effects |
|
Topical corticosteroid containing
antifungal preparation should be avoided even for an inflammatory lesion |
Topical antifungals with anti-inflammatory
effect can be used |
|
Keratolytics and Whitfield’s ointment can
be used in the treatment of glabrous tinea |
Should be avoided if there is local
inflammation |
|
Antifungal (with few exceptions) should be
applied twice a day |
Twice a day application is required to
achieve good clinical response |
|
Treatment may be continued for about 2
weeks after clinical resolution |
Clinical cure may not correspond with
mycological cure |
|
Topical formulation could be chosen
according to the site involved |
There are advantages of certain
preparations; Eg. lotions in hair-bearing area |
|
There is no added advantage in the efficacy
of various formulations like lotions and sprays over the creams |
Most of these preparations have advantage
of being user friendly but not of added efficacy |
|
Various classes of topical antifungals
currently available are nearly equipotent |
Few studies on head-to-head comparison of
topical antifungals are published, but still the evidence is not sufficient
to consider one molecule is superior to the other |
|
No role for use of combination of two
topical antifungals |
No studies to substantiate benefits of such
a combination approach and it is not practiced routinely |
These
recommendations are based not entirely on evidence but on consensus for the
current scenario of recalcitrant dermatophytosis.
Topical antifungal therapy is integral to the
management of glabrous tinea especially in the setting of localized infection,
pregnancy, and children and in the presence of some co morbidities when
systemic antifungals cannot be used. Topical antifungals can be useful
adjuvants to systemic antifungals in the current scenario as they may have an
additive effect and achieve high local concentration. Reaction at the site of
application is rare and is the only significant adverse effect.
The ideal topical antifungal agent should
have a high cure rate, low relapse rate and minimal adverse effects. Extensive
infection and high cost, especially of the newer topical antifungals, are
limitations to topical therapy.
The type of topical formulation could be chosen according to the
site involved. Topical agents are available as creams, ointments, lotions,
sprays, gels, powders and soaps. Lotion and spray formulations were not
considered more effective than creams, although they may be more convenient
when larger areas are involved. However, a potential for irritation and high
cost are the disadvantages of these products. Antifungal soaps and powders are
not recommended in the management of glabrous tinea.
A combination of systemic and topical
antifungal drugs is essential in the treatment of glabrous tinea, with the
extent of disease being a limiting factor for topicals. There was no consensus
regarding the superiority of one topical antifungal over another and whether
they should be from the same or different group as the oral antifungal
prescribed. As dermatophytes are keratinophilic, moving radially, the topical
antifungal should be applied inward, from beyond the margin of the lesion.
Application may be continued twice daily until 2 weeks after achieving clinical
resolution of lesions. There was no consensus on the routine use of combination
of two topical antifungals.
There is no role for corticosteroids alone or in combination with
antifungals in the management of dermatophytosis of the glabrous skin including
inflammatory tinea. There was no consensus on gradual withdrawal of topical
steroid in corticosteroid modified tinea.
In India, topical antifungal, antibacterial and corticosteroid
combination creams containing 3-5 components (viz. a potent corticosteroid like
clobetasol propionate, ornidazole, ofloxacin and an antifungal agent) are
unfortunately freely available over-the-counter. They are often used for the
treatment of tinea corporis, tinea cruris and tinea faciei, leading to a
variety of adverse effects. Antifungal without any corticosteroid or
antibacterial only should be used for the treatment of glabrous tinea. Topical
corticosteroids should never be used for tinea corporis, tinea cruris or tinea
faciei. Some classes of topical antifungals such as azoles and allylamines have
anti-inflammatory properties due to their inhibitory effects on cytokines and
may be useful for treating patients with inflammatory lesions and
corticosteroid modified tinea.
Keratolytics have been used for the treatment of dermatophytosis,
especially hyperkeratotic tinea pedis. Topical keratolytics, such as
Whitfield's ointment (3% salicylic acid with 6% benzoic acid), can be used in
the treatment of glabrous tinea, but not on the flexures or face or where the
lesions are inflamed.
Most topical antifungals need to be applied twice daily, but
luliconazole and terbinafine may be applied once daily. Clotrimazole,
miconazole, oxiconazole and ketoconazole are relatively less expensive.
Topical
antifungal preparations available in India
|
Class |
Drug
name |
Preparations |
FDA
Pregnancy Category |
|
Imidazoles |
Ketoconazole |
2
% cream, powder, lotion (with or without1% zinc pyrithione), soap |
C |
|
Miconazole
nitrate |
2
% cream, gel, powder |
C |
|
|
Clotrimazole |
1
% cream, lotion, powder, soap |
B |
|
|
Oxiconazole |
1
% cream, lotion |
B |
|
|
Fenticonazole |
2
% cream |
Not
categorized |
|
|
Bifonazole |
1
% cream |
B |
|
|
Eberconazole |
1
% cream |
C |
|
|
Sertaconazole
nitrate |
2
% cream, lotion |
C |
|
|
Luliconazole |
1
% cream, lotion, spray |
C |
|
|
Triazoles |
Fluconazole |
0.5
% gel, powder |
C |
|
Allylamines |
Terbinafine
hydrochloride |
1%
cream, gel, powder, lotion |
B |
|
Benzylamines |
Butenafine |
1%
cream |
B |
|
Morpholenes |
Amorolfine
hydrochloride |
0.25
% cream, 5 % nail lacquer |
Not
categorized |
|
Hydroxy-pyridinone |
Ciclopirox
olamine |
8%
Nail lacquer, 1% cream, 1% shampoo |
B |
|
Others |
Tolnaftate |
Solution(10mg/ml),
cream (10mg/g) |
Not
assigned. To be used if benefits outweigh risk. |
|
Whitfield’s
ointment |
3%
salicylic acid and 6% benzoic acid in ointment base |
C
(due to risk of absorption of salicylic acid) WHO allows application,
especially if benefits outweigh risks |
Specific
characteristics of relatively newer select topical antifungals available in
India
|
Drug |
Class |
Remarks |
|
Terbinafine |
Allylamine |
Fungicidal
antifungal as compared to fungistatic nature of most other antifungals |
|
Butenafine |
Benzylamine |
Fungicidal
antifungal as compared to fungistatic nature of most other antifungals |
|
Bifonazole |
Imidazole |
Dual
mode of action by inhibition of 14α-demethylase and microsomal
HMG-CoA-reductase leading to fungicidal effect |
|
Sertaconazole |
Imidazole |
Anti-inflammatory
action. Contains a benzothiophene ring which mimics tryptophan and increases
the drug’s ability to form pores in the fungal cell membrane |
|
Eberconazole |
Imidazole |
Potent
anti-inflammatory activity. |
|
Luliconazole |
Imidazole |
Reservoir
effect. Highest antifungal activity against Trichophyton spp.
among currently available topical antifungal drugs. |
|
Fenticonazole |
Imidazole |
Additional
action of blocking cytochrome oxidases and peroxidises. |
|
Amorolfine |
Morpholine |
New
class of antifungal with different mechanism of action mediated through
inhibition of two different enzymes. |
|
Ciclopirox
olamine |
Hydroxypyridinone |
Acts
through chelation of metal ions (Fe3+); inhibits cytochrome oxidase, catalase
and peroxidase resulting in intracellular degradation of toxic peroxides;
inhibits cellular uptake of essential compounds and alters cell permeability |
Topical corticosteroid application adversely
affects the epidermal barrier function by increasing transepidermal water loss
and decreasing the ceramide content of the stratum corneum. Hence, emollient
application should be encouraged, particularly in patients with corticosteroid
modified tinea, to enhance the barrier function and provide symptomatic relief.
Antihistamines can be used to alleviate pruritus. There are a few reports
supporting the use of antifungal powders in tinea pedis, but antifungal powders
are not recommended for other forms of tinea.
Systemic
therapy
Recommendation of Systemic
treatment of glabrous tinea (tinea corporis, tinea cruris and tinea faciei)
|
Antifungal |
Dose |
Minimum duration |
Precautions |
|
|
|
||||
|
Children |
Adults |
|||
|
Itraconazole |
3-5mg/kg/day |
Naïve: 100 mg 1 or 2 capsules od |
3 weeks |
Drug interactions, hepatotoxicity |
|
CH/SMT/RCL: 100mg bd/ 100 mg 2 od |
4 weeks |
|||
|
Terbinafine |
10-20 kg - 62.5 mg |
Naïve: 250mg/day |
4 weeks |
Skin rash, hepatotoxicity |
|
20-40 kg- 125 mg |
CH/SMT/RCL: 250 mg bd / day |
4 weeks |
||
|
Griseofulvin |
10-20 mg/kg/day |
Naïve: 500 mg/day |
8 weeks |
GI intolerance, head ache |
|
CH/SMT/RCL: 750 -1000 mg/ day |
8 weeks |
|||
|
Fluconazole |
3-6 mg/kg/day |
Naïve: 50-100 mg/day |
4 weeks |
Hepatotoxicity |
|
150-300 once weekly |
8 weeks |
|||
|
CH/SMT/RCL: 100 mg/day |
6 weeks |
|||
|
150 mg /thrice weekly* |
8 weeks |
|||
Note: Some of the dose schedules in children have been
extrapolated from their uses in conditions like tinea capitis. Pediatric dose
should not exceed the adult dose. References hold good for some of the drug
dosages and not the duration. Duration of therapy is best individualized based
on the clinical response. *Dosage in current practice and not evidence based.
CH- Chronic; SMT - Steroid modified tinea; RCL -Recalcitrant
Consensus recommendation for
the various facets of treatment of glabrous tinea
|
Comments |
Recommendation |
|
|
Indications |
||
|
Glabrous tinea |
Most cases in the current scenario require
systemic therapy |
Involvement of multiple sites |
|
Extensive disease based on clinical
judgement |
||
|
Chronic dermatophytosis |
||
|
Recurrent dermatophytosis |
||
|
Steroid modified dermatophytosis/ Tinea
incognito |
||
|
Failure of topical therapy |
||
|
Associated nail and hair involvement vellus hair involvement by dermatoscopic
examination |
||
|
Immunocompromised states like hematological
malignancies and therapy with immunosuppressive drugs |
||
|
Choice of systemic drug |
||
|
First line |
Best option considering overall efficacy
and safety |
Itraconazole, Terbinafine, |
|
Alternate drugs |
Prolonged duration of treatment required |
Griseofulvin, Fluconazole |
|
Complementary topical therapy |
||
|
Choice and rationale |
Topical antifungal without corticosteroid
and antibacterial components. |
Systemic antifungal therapy should
preferably be combined with topical antifungal therapy which may be of same
or different class |
|
There are limited laboratory/clinical
studies on the efficacy and utility of combination antifungals (systemic with
topical OR two systemic) for dermatophytosis of the glabrous skin |
||
|
Response |
||
|
Failure |
No improvement or worsening of symptoms and
signs at 3 weeks |
Assessment of factors responsible for it
and if detected to be corrected; if not, antifungal therapy to be changed |
|
Total response |
Complete subsidence of symptoms and signs
with or without post-inflammatory changes anytime during the treatment |
Completion of therapy for the stipulated
period or as per the individual response |
|
Partial Response |
Partial subsidence of symptoms and signs at
the end of 3 weeks |
Extended duration of treatment to be
considered with appropriate laboratory monitoring; double dosing of
terbinafine may be considered |
|
Cure |
||
|
Clinical cure |
Complete subsidence of symptoms and signs
with or without post-inflammatory changes at the end of treatment |
Follow up must be at 4 weeks after apparent
clinical cure to look for recurrence |
|
Mycological cure |
Complete subsidence of symptoms and signs
with negative mycology reports (direct microscopy with/without culture) at
the end of the treatment |
Follow up must be at 4 weeks after apparent
clinical cure to look for recurrence |
|
Laboratory monitoring |
||
|
Hepatotoxicity |
All systemic antifungals are hepatotoxic |
Monitoring hepatic function if the
treatment is extended or if the dose is doubled |
|
Renal toxicity |
Systemic drugs used in the management of
dermatophytosis do not commonly cause renal toxicity |
Renal monitoring may be considered if
indicated on clinical grounds |
|
Follow up |
||
|
First follow up visit |
To assess clinical response |
At 3 weeks, if inadequate response |
|
Final follow up visit |
To assess recurrence |
At 4 weeks after apparent clinical cure |
|
Special situations |
||
|
Pregnancy |
Teratogenicity of the drugs should be
addressed |
Topical antifungals with established safety
|
|
Oral terbinafine (routine use should be
avoided) |
||
|
Lactating mother |
Safety of the infant should be addressed |
Topical antifungals |
|
Oral fluconazole |
||
|
Children under 2 years |
Safety with respect to hepatotoxicity, GI
intolerance and other adverse effects should be addressed |
Topical antifungals with established safety |
|
Oral fluconazole |
||
|
Children above 2 years |
Safety with respect to hepatotoxicity, GI
intolerance and other adverse effects should be assessed |
Topical antifungals with established safety |
|
Oral terbinafine, itraconazole, fluconazole
and griseofulvin |
||
|
Hepatic dysfunction |
Monitoring of the hepatic function is mandatory |
Topical antifungals |
|
Oral fluconazole |
||
|
Renal dysfunction |
Renal function monitoring if terbinafine is
used (dose reduction if creatinine clearance is <50 ml/ min) |
Topical antifungals |
|
Oral itraconazole |
||
|
Cardiac dysfunction |
Cardiotoxicity of drugs should be addressed |
Topical antifungals |
|
Oral terbinafine |
||
Patients on systemic antifungals should be
regularly followed to ensure adherence to treatment and to monitor the
therapeutic response. The first follow up visit should be at the end of 3 weeks
to assess the clinical response. If there is partial response (i.e. persistent
pruritus and incomplete/minimal resolution of lesions), therapy should be
continued while reassessing for contributing factors. If there is no response,
change of the antifungal drug should be considered. Regular follow up should be
continued both during treatment and at least up to 4 weeks after apparent
clinical cure.
Standard indications for systemic therapy in dermatophytosis are
extensive disease, involvement of multiple sites, recurrence, chronicity,
failure of topical therapy, nail or hair involvement, vellus hair involvement
on dermatoscopy and immunocompromised status. In India, now days, most patients
require a combination of systemic and topical antifungal drugs for a longer
duration than that is conventionally recommended. This is particularly true for
patients with corticosteroid modified, chronic, recurrent or recalcitrant
infection. Persistent papules or nodules in a healing or unresponsive lesion
may indicate Majocchi granuloma, which also needs prolonged treatment. The
duration of treatment may be individualized based on clinical response. The end
point of treatment for glabrous tinea should be the achievement of clinical
cure.
Terbinafine may be used as first line therapy in treatment-naïve
and terbinafine-naïve patients with glabrous tinea. If there is an inadequate
response at the end of 3 weeks of terbinafine 250 mg once a day, increasing the
dose to 250 mg twice daily may be considered in adult patients, albeit with
monitoring of liver function.
Terbinafine 250 mg daily or itraconazole 200 mg daily in adults
for 4-6 weeks have been recommended for treatment of chronic, widespread
dermatophytosis. Griseofulvin 500-1000 mg daily taken after fatty meal until
cure (3-6 months) has been mentioned as an alternative drug. Itraconazole and
terbinafine are especially useful in sebum rich areas, as the skin
pharmacokinetics (pK) are determined predominantly by their lipophilicity.
Experts agreed that griseofulvin and fluconazole need to be taken
for a longer duration than itraconazole or terbinafine.
There have been concerns over increasing instances of failure to
terbinafine in tinea corporis, tinea cruris and tinea faciei in the country.
Resistance to terbinafine due to mutations in the squalene epoxidase (SQLE) gene of Trichophyton interdigitale and T.
rubrum has been documented in studies from Chandigarh and New
Delhi. High MIC's (Minimum inhibitory concentration) were observed and a higher
dose (250 mg twice daily) or increased duration was found to be more effective
in a study, hence the authors concluded that increased exposure to terbinafine,
resulting in higher levels of the drug in the stratum corneum, could offset the
higher MIC and the effect of SQLE mutation
to some degree.
Itraconazole may be used as a first line option or when there is
no response to terbinafine and is now the most commonly prescribed oral
antifungal agent for dermatophytosis. It should be taken immediately after food
or with aerated beverages or acidic juice to improve its bioavailability. While
the standard dosage for glabrous tinea is 100 mg once daily for 15 days or 200
mg (as 2 capsules of 100mg taken together or in a BD dose) for 1 week, the
current scenario calls for individualization of the duration based on clinical
response and continuation of treatment until achieving cure. The experts agreed
on not using the unapproved higher dose formulations of itraconazole.
Different brands of itraconazole available in India vary in the
pellet morphology and thereby the resultant quality and therapeutic effect. The
drug-polymer ratio, polymer type, coating thickness, bead size and number
determine the dissolution of a capsule of itraconazole. Morphometric analysis
of pellets using dermoscopy is a simple method to quantify the quality of a
brand of itraconazole. A recent study stated that a pellet count of ≥560 (100
mg capsule) provides a surface area comparable to the innovator brand and may
be taken as a cut off for distinguishing poor quality brands. In a compliant
patient whose disease is not responsive, changing to a better brand is
justified. Since itraconazole follows non-linear pharmacokinetics, a dose
higher than 200 mg daily may result in decreased clearance and eventually toxic
levels.
In some parts of India, dermatologists have found good therapeutic
response to griseofulvin given for 6-8 weeks although not consistently. Since
the levels are high in the stratum corneum, this drug could be especially
useful in patients prone to increased sweating.
The standard dose of fluconazole in adults is 150-300 mg weekly
for 4-6 weeks or 50-100 mg daily 4 weeks. However, it is being commonly
prescribed in the dose of 150 mg thrice weekly (extrapolated from the regimen
for complicated vulvovaginal candidiasis) in certain parts of India with good
results. Skin pharmacokinetic (pK) studies have found that its skin levels are
markedly higher with a dose of 100 mg given daily. Notably, fluconazole
achieves high levels in stratum corneum, reaching there mainly by way of direct
diffusion. Thus, its pathway of reaching the corneum is different from
terbinafine and itraconazole which largely depend on sebum secretion and this
makes it potentially useful in patients with dry skin and in children who have
lesser sebum secretion than adults. However, a disadvantage is that the levels
decrease rapidly following treatment discontinuation due to low keratin
adherence.
There is paucity of literature with regard to the use of
combination of oral antifungals in the treatment of dermatophytosis. Such
combinations need to be first assessed in laboratories by checkerboard studies
for synergistic activity before considering any clinical utility. Although few
studies have proven synergistic effect of combination antifungal therapy
against dermatophytes, more evidence is desirable.
Ketoconazole is an imidazole compound with a
mechanism of action similar to that of triazoles. It had been used in the
management of glabrous tinea in a dose of 200-400 mg daily in adults. It is no
longer approved by US FDA for the management of superficial fungal infections
because of hepatotoxicity, which may be asymptomatic or can present as acute
liver injury. Though available in India, it is not recommended for routine use,
but is to be used only as a reserve drug with close monitoring of liver
function.
There was no consensus for statements such as use of systemic
antifungals in all cases of tinea faciei, initiation of terbinafine in 250 BD
dosages, use of fluconazole and griseofulvin as first line therapy or of
ketoconazole as a reserve drug. There was also no consensus on updosing of
itraconazole and standard fixed duration of therapy for glabrous tinea
infection.
Systemic therapy
should be continued for another 2 weeks after clinical resolution in
recalcitrant cases. Since some systemic antifungal drugs can cause
hepatotoxicity, it is advisable to do baseline LFTs to rule out impaired liver
function and periodic follow-up, if the treatment duration exceeds 4 weeks,
especially in recalcitrant cases, and in the elderly, while it is not mandatory
in naïve cases.
Special situations
Dermatophytosis is now the commonest
dermatologic condition seen among outpatients in India. Co morbidities such as
diabetes, anemia and immunosuppressive diseases or immunosuppressive therapy,
may alter the clinical presentation and predispose such patients to
recalcitrant or recurrent infections.
Treatment of dermatophytosis in pregnancy, lactating women,
infants, children and geriatric patients has certain limitations.
Corticosteroid-modified tinea
Corticosteroid-modified tinea and tinea incognito have become
common presentations. Some patients tend to apply the topical corticosteroid
antibacterial antifungal combination creams continuously or intermittently over
weeks to months and present with morphological variants such as tinea
pseudoimbricata and breakthrough lesions. Studies have shown that application
of more than 50 gm of 0.05% clobetasol propionate per week can result in
adrenal suppression. Hence, it is quite understandable that patients may
present with Cushingoid features and a low serum cortisol level. Literature
states that the recovery of the hypothalamus takes about 14-30 days after
cessation of corticosteroids. This explains the delay in clinical response seen
in patients with steroid modified dermatophytosis, who will hence require an
extended duration of treatment. Patients with steroid modified dermatophytosis
with Majocchi granuloma have been shown to achieve clearance with the use of
pulse therapy with itraconazole given as 200 mg BD for 7 days followed by drug
free period of 14 days (up to 3 pulses).
Pregnancy and lactation
The ideal management of glabrous tinea during pregnancy is by
using only safer topical antifungals. Though oral terbinafine is a FDA
pregnancy category B drug, scarce human data precludes its routine use in
pregnancy until safety data is available. Itraconazole and griseofulvin, both
belong to category C, while fluconazole is a category D drug (except as a 150
mg single dose). Among the topical antifungals, clotrimazole, oxiconazole,
bifonazole, terbinafine and ciclopirox olamine belong to Category B, while the
newer azoles such as sertaconazole, eberconazole and luliconazole are category
C drugs. Systemic absorption is considered to be very low with amorolfine and
hence it may be safely used in pregnancy.
All topical antifungals can be used safely during lactation as
their secretion in milk is negligible. Cream, gel or liquid products which are
water miscible are recommended for application to the skin over the breast
because ointments may expose the infant to mineral paraffin while feeding. Data
regarding the use of systemic antifungals including terbinafine during
lactation is scarce, and therefore they should be avoided as far as possible
especially in mothers of preterm infants. However, fluconazole has an
acceptable safety profile as its secretion in the breast milk is low. Experts
recommend that the decision on treatment should be based on the given clinical
scenario.
Infants and children
Glabrous tinea infections have become common in children in the
recent times. There are differences in epidemiology, host biology, predisposing
factors and clinical presentation in children as compared to adults. Topical
antifungals can be given safely in children since their percutaneous absorption
is negligible. Use of topical corticosteroid-antifungal combination creams
result in early deleterious effects on the skin of children and persistence of
infections and thus is to be avoided.
Localized infection may be treated with topical antifungals alone.
However, recurrent, chronic or corticosteroid modified tinea, which is being
increasingly observed in children, warrants the use of systemic antifungals.
The dosage of systemic antifungals should be based on the body weight.
Antifungals like griseofulvin, terbinafine and itraconazole can be used in
children above 2 years of age to treat glabrous tinea infections. Considering
the safety aspects, fluconazole may be the preferred systemic antifungal in
infants and children below 2 years of age. Secretion and distribution pattern
of this drug is not dependent on sebum and directly diffuses into the skin.
Elderly persons
Physiological, psychological and socioeconomic factors, co
morbidities (renal, hepatic, cardiac) and influence of polypharmacy should be
considered while treating elderly patients. A healthy elderly patient may be
treated in the same manner as a young adult. Changes in pharmacokinetics must
be considered while deciding an appropriate antifungal drug in elderly patients
with altered hepatic or renal functions. It is very important to check for
various drug interactions before treating elderly patients on polypharmacy.
Systemic co morbidities
Appropriate laboratory monitoring is mandatory in patients with
known hepatic and renal dysfunction while using systemic antifungals. No
recommended dose adjustment is available for systemic antifungals in patients
with hepatic impairment. Monitoring them regularly is the only option.
Fluconazole, as compared to other triazoles, is characterized by high water
solubility and the drug is primarily eliminated by the kidneys. Hepatic
metabolism does not seem to play an important role in the elimination of the
drug. Oral fluconazole with laboratory monitoring can hence be considered as a
relatively safer drug in patients with hepatic dysfunction. Itraconazole is
eliminated mainly through feces and in lesser amount through the urine. Oral
itraconazole is thus a safer drug in patients with renal dysfunction.
Itraconazole has however been associated with congestive cardiac failure and
must be avoided in patients predisposed to the same. Oral terbinafine is a
relatively safer drug in patients with cardiac dysfunction. However, in
patients with renal dysfunction, the dose needs modification if creatinine
clearance is <50 ml/minute.
N.B Topical azoles may
be considered for use in pregnancy, whereas all oral antifungals are better
avoided, especially in the first two trimesters. Topical azoles and oral
fluconazole may be used in lactation. In neonates, topical azoles and oral
fluconazole are safely used, whereas in older children, all topical and oral
antifungals are safe for use, provided accurate dose adjustment is done.
Drug interactions
Systemic antifungals should be used
appropriately in patients on polypharmacy after checking for various drug
interactions. Terbinafine has the least drug interactions and is generally
the preferred choice of drug in patients on polypharmacy.
Clinically relevant drug
interactions with antifungals
|
Antifungal drug |
Drug level is decreased by |
Decreases level of these drugs |
Increases level of these drugs |
|
Griseofulvin |
Phenobarbital |
Anticoagulants, oral contraceptives,
Cyclosporin |
Potentiates action of alcohol-Disufiram
like reaction |
|
Terbinafine |
Rifampicin |
- |
Anti-depressants beta blockers, |
|
Antiarrthymics class 1c, selective
serotonin reuptake inhibitors. |
|||
|
Caution when used with anticoagulants. |
|||
|
Itraconazole |
H2 histamine blockers, proton pump
inhibitors, rifampicin, rifabutin, INH, ritonavir, nevirapine, nortriptyline,
carbamazepine, phenytoin, phenobarbital |
Oral contraceptives |
Glibenclamide, phenytoin, warfarin,
cyclosporin, tacrolimus, digoxin, lovastatin, midazolam, triazolam,
methylprednisolone, Saquinavir |
|
Fluconazole |
Rifampicin |
Oral contraceptives |
Sulfanylurea, nifedipine, theophylline,
NSAID, warfarin, cyclosporine |
BRITISH ASSOCIATION OF
DERMATOLOGISTS’ GUIDELINES FOR THE MANAGEMENT OF TINEA CAPITIS 2014
Definition
Tinea capitis is an infection of scalp hair follicles and
the surrounding skin, caused by dermatophyte fungi, usually species in the
genera Microsporum and Trichophyton.
Epidemiology and etiology
Tinea capitis is predominantly a disorder of prepubertal
children. Although Microsporum canis remains the most commonly involved
organism, a shift towards anthropophilic species continues to be observed.
Trichophyton tonsurans is reported to account for 50–90% of dermatophyte scalp
isolates in the U.K. This rise in anthropophilic dermatophyte infections is
attributed to immigration and travel patterns.
Laboratory diagnosis of tinea capitis
Although the clinical diagnosis of tinea capitis is often
relatively accurate, when considered, laboratory investigations to confirm the
diagnosis are advisable to isolate the causal organism and direct the choice of
systemic therapy. Post-treatment samples should be sent to ensure clearance.
Taking specimens
Suspected tinea capitis lesions should be sampled either
by plucking hairs, using a blunt scalpel to remove hair and scalp scale, or by
taking scalp brushings. In cases of tinea capitis caused by M. canis, affected
hairs identified by fluorescence under a Wood’s lamp may be plucked and
constitute an appropriate specimen. Specimens should be collected in paper or
card packs. A disadvantage of brush sampling is that it does not enable the
laboratory to examine the specimen microscopically and permits only culture.
Friedlander et al. have demonstrated that gauze swabs make an equally effective
and often more convenient sampling method. It is considered that sampling the
edge of scalp lesions may provide higher yields of causal fungus. Sampling of
kerions may be problematic, and culture is often negative. A swab of the lesion
may provide the most appropriate specimen.
Scalp lesions in suspected cases of tinea capitis should
be sampled by scalpel scraping, hair pluck, brush or swab as appropriate to the
lesion.
Laboratory investigations
Microscopy should be carried out on all scalp scrapings
and plucked hairs, by mounting in 10–30% potassium hydroxide with or without
calcofluor, and examination by light. The presence of hyphae and/or
arthroconidia should be reported. Where
possible it should be determined whether the arrangement of arthroconidia is
endothrix or ectothrix, but this is often difficult. All specimens should be
cultured on Sabouraud agar with at least one agar plate containing
cycloheximide to inhibit nondermatophyte mould growth. Plates should be
incubated for at least 2 weeks. Where exposure to cattle is documented and an
infection caused by T. verrucosum is suspected, plates should be incubated for
up to 3 weeks and examined very carefully at the end of this period for the
presence of the slow-growing and inconspicuous colonies of this species. Any
dermatophytes growing should be identified and reported.
All specimens from cases of tinea capitis should be
processed for microscopy and culture where possible, and the causal agent fully
identified where isolated. Susceptibility testing is not indicated.
Management
The aims of treatment are eradication of the organism,
resulting in both a clinical and mycological cure as quickly and safely as possible;
alleviation of symptoms; prevention of scarring and reduction of transmission
to others. Oral therapy is generally required to achieve these goals.
When to start treatment
Ideally one should wait for confirmation of the presence
of fungus, either by conducting microscopy at the patient side or waiting for
culture. However, in high-risk populations, awaiting results increases delay
(as culture results may take 2–4 weeks to be available) and may further
increase spread. So, in the presence of a kerion or when the diagnosis of a
fungal infection is strongly suspected clinically based on the presence of very
typical features of scaling, lymphadenopathy or alopecia, it is reasonable to
start therapy immediately, as these are strong predictive factors for tinea
capitis.
Topical therapy
Topical therapy alone is not recommended for the
management of tinea capitis. However, topical agents such as povidone–iodine,
ketoconazole 2% and selenium sulfide 1% shampoos are used to reduce
transmission of spores.
Oral therapy
It is reasonable to begin treatment on the basis of one
or more cardinal signs, while awaiting confirmatory mycology. Treatment protocols should be based on the
most likely culprit organism. A prolonged course or a change of agent may be required
in cases of treatment failures, or if an unexpected fungus is identified on
culture. Although griseofulvin remains the only licensed treatment for tinea
capitis in children, cumulative evidence now demonstrates that newer antifungal
agents have higher response rates, and are safe and more cost-effective.
Choice of drug according to organism isolated
Trichophyton tonsurans:
Terbinafine
Trichophyton violaceum, soudanense: Terbinafine
Microsporum canis:
Griseofulvin or itraconazole
Microsporum audouinii:
Griseofulvin or itraconazole
Griseofulvin
Griseofulvin is a fungistatic drug that inhibits nucleic
acid synthesis, arrests cell division at metaphase and impairs synthesis of the
cell wall. It is available in several
forms (micronized, ultra micronized and suspension).
The standard licensed treatment protocol for those aged
> 1 month is 1 g in children weighing > 50 kg, or 15– 20 mg/ kg daily in
single or divided doses for 6–8 weeks if < 50 kg. Taking the drug with fatty
food may increase absorption and improve bioavailability. Dosage
recommendations vary according to the type of formulation used and how easily
it is absorbed. It may be necessary to use doses up to 25 mg/ kg daily for more
prolonged periods in resistant cases.
Side-effects occur in 20% of cases, mostly
gastrointestinal upset, in particular diarrhea, rashes and headache. The drug
is contraindicated in pregnancy and men are cautioned against fathering a child
for 6 months after treatment.
Advantages: extensive experience; suspension more
palatable to children and allows more accurate dosage adjustments.
Disadvantages: increasingly expensive; prolonged
treatment required with potential to affect compliance.
Contraindications: lupus erythematosus, porphyria, severe
liver disease.
Drug interactions: include warfarin, ciclosporin and the
oral contraceptive pill.
Terbinafine
Terbinafine is an allylamine that acts on the cell
membrane and is fungicidal. It shows activity against all dermatophytes, but
has much higher efficacy against Trichophyton species than Microsporum. Additionally, terbinafine is not excreted in
the sweat or sebum of prepubertal children, and cannot be incorporated into the
hair shaft in children, so does not effectively reach the scalp surface where
the arthroconidia are located in Microsporum infections, accounting for its
relative inefficacy. In contrast, meta-analysis of RCTs shows that 2–4 weeks of
terbinafine is at least as effective as 6–8 weeks of griseofulvin in T.
tonsurans infections. Terbinafine may now be considered the optimal choice,
when cost-efficiency and compliance are taken into account.
Pharmacokinetic studies of terbinafine show that children
require significantly weight-normalized doses to approximate the equivalent
drug levels needed for efficacy in adults. Terbinafine appears well tolerated
in children.
Side-effects include gastrointestinal disturbances and
rashes in < 8%.
Advantages: fungicidal; shorter treatment regimens, so
potential to improve compliance; cost; safety.
Disadvantages: no suspension formulation
Drug interactions: plasma concentration is decreased by
rifampicin and increased by cimetidine.
Itraconazole
The primary mode of action of Itraconazole is
fungistatic, through depletion of cell-membrane ergosterols, which interferes
with membrane permeability. A dose of 50–100 mg daily for 4 weeks or 5 mg/ kg
daily for 2–4 weeks is used. Itraconazole is now the preferred agent as it has
activity against both Microsporum and Trichophyton species. The drug is well
tolerated and has been shown to be safe for use in the first year of life.
Intermittent dosing regimens are effective and may be
preferred. Advantages: pulsed regimes;
shorter treatment protocols; available in liquid form.
Drug interactions: enhanced toxicity of warfarin, some
antihistamines (specifically terfenadine, astemizole), antipsychotics
(sertindole), anxiolytics (midazolam), digoxin, cisapride, ciclosporin and
simvastatin (increased risk of myopathy); decreased efficacy with concomitant
H2 blockers, phenytoin and rifampicin.
Fluconazole
Fluconazole has been used in the treatment of tinea
capitis and has been advocated as an alternative to terbinafine. Once-weekly dosing regimens have been used
and appear well tolerated.
Additional measures
Exclusion from school
Although the potential risk of transmission of infection
to unaffected classmates has led some authorities to recommend exclusion from
school, most experts consider this impractical and suggest that children
receiving appropriate systemic and adjunctive topical therapy should be allowed
to attend school.
Family screening
Index cases due to the anthropophilic T. tonsurans are
highly infectious. More than 50% of family members (including adults) may be
affected, often with occult disease. Failure to treat the whole family will
result in high recurrence rates. Therefore we recommend screening of all family
members and treating those found positive.
Cleansing of fomites
Viable spores have been isolated from hairbrushes and
combs. For all anthropophilic species, these should be cleansed with disinfectant.
This has particular implications for barbers, who need to ensure that
appropriate measures are taken to disinfect multiuser equipment. Disinfectants
commonly used are simple bleach or a 2% aqueous solution of sodium hypochlorite
containing 16.5% salt.
Steroids
The use of corticosteroids (both oral and topical) for
inflammatory varieties of tinea capitis (e.g. kerion and severe id reactions)
may reduce itching and general discomfort, but is controversial. Historically,
oral steroids were thought to reduce scarring, but studies show that, compared
with oral antifungal therapy alone, they do not reduce the time to clearance,
and therefore confer no long-term advantage, so are not recommended. Scarring is rare in T. tonsurans infection,
and hair usually fully regrows after effective oral antifungal therapy alone.
Treatment failure
Some individuals are not clear at follow-up. The reasons
for this include (i) lack of compliance – especially in long treatment courses;
(ii) suboptimal absorption of drug; (iii) relative insensitivity of the
organism; and (iv) reinfection. If fungi can still be isolated at the end of
treatment, but the clinical signs have improved, it is reasonable to continue
therapy for a further 2–4 weeks. However, if there has been no clinical
response, it is imperative to ensure that the antifungal therapy is appropriate
for the causal organism identified on culture. If so, the options then are (i)
to increase the dose or duration of the original drug; or (ii) to change to an
alternative agent, for example griseofulvin to itraconazole (for M. canis);
terbinafine to itraconazole (for T. tonsurans); or itraconazole to terbinafine
(for T. tonsurans).
Carriers
In asymptomatic carriers (i.e. those individuals without
overt clinical infection who are culture positive) with a high spore load, oral
therapy is usually justified. If the spore load is low, carriage may be
eradicated with topical treatment alone, but close follow-up is needed, with
repeat mycology, to ensure that treatment has been effective.
Follow-up
The definitive end point for adequate treatment must be
mycological cure, rather than clinical response. Therefore, follow-up with
repeat mycology sampling is recommended at the end of the standard treatment
period and then monthly until mycological clearance is documented. Treatment
should therefore be tailored to each individual patient according to response.
SUMMARY OF TREATMENT CHOICE
Laboratory diagnosis
Scalp lesions in suspected cases should be sampled via
scalpel scraping, hair pluck, brush or swab. All specimens should be processed
for microscopy and culture, where possible. Susceptibility testing is not
indicated.
Treatment
In the presence of a kerion or where one or more of the
cardinal clinical signs is present (scale, lymphadenopathy, alopecia) it is
reasonable to commence treatment while awaiting confirmatory mycology.
Topical therapy alone is not recommended for the
treatment of tinea capitis. Oral therapy is generally indicated to achieve both
clinical and mycological cure. Choice of systemic therapy should be directed by
causative dermatophyte.
First-line therapy
Both griseofulvin and terbinafine have good evidence of
efficacy and remain the most widely used first-line treatments. As a general
rule, terbinafine is more efficacious against Trichophyton species (T.
tonsurans, T. violaceum, T. soudanense), and griseofulvin more effective
against Microsporum species (M. canis, M. audouinii). Terbinafine requires a
shorter course of treatment, which may increase compliance.
Griseofulvin dose by body weight
< 50 kg 15–20 mg /kg per day (single or divided dose)
for 6–8 weeks
> 50 kg 1 g per day (single or divided dose) for 6–8
weeks
Doses up to 25 mg/kg per day may be required in some
cases
Terbinafine dose by body weight
< 20 kg 62.5 mg per day for 2–4 weeks
20–40 kg 125 mg per day for 2–4 weeks
> 40 kg 250 mg per day for 2–4 weeks
Treatment failure
Initially consider lack of compliance, suboptimal
absorption of drug, relative insensitivity of the organism and reinfection. In
cases of clinical improvement but ongoing positive mycology, continue current
therapy for a further 2–4 weeks. If there has been no initial clinical
improvement, proceed to second-line therapy below
Second-line therapy
Itraconazole is safe, effective and has activity against
both Trichophyton and Microsporum species. If itraconazole has been selected as
first-line therapy, convert to terbinafine second line for Trichophyton
infections or griseofulvin for Microsporum species, at standard dosing
regimens.
Itraconazole, 50–100 mg per day for 4 weeks, or 5 mg/ kg
per day for 2–4 weeks
Alternative agents
For cases refractory to the above regimens, other
modalities to be considered in exceptional circumstances include fluconazole.
Additional measures
Children receiving appropriate therapy should be allowed
to attend school.
Index cases due to T. tonsurans warrant screening of all
family members and close contacts and treatment for those positive cases.
In asymptomatic carriers (no clinical infection, culture
positive) with a high spore load, systemic treatment is generally justified.
The end point of treatment is mycological rather than
clinical cure; therefore repeat mycology sampling is recommended until
mycological clearance is achieved.